Straumann® Emdogain: Indications for the surgical procedure
- Periodontal surgical procedure for intraosseous defects (Prof. Anton Sculean: “For the treatment of periodontal intrabony defects, we have the best possible evidence”)1 and
- in the case of broad intraosseous defects in combination with bone substitute materials, in addition to
- mandibular furcation defects (grade I and grade II furcation) and
- recession defects (Miller grades 1 to 3).
Emdogain® is also indicated for oral wound healing (e.g. the use of Emdogain® to enhance the wound healing in implant procedures) and surgical therapy of peri-implant disease (peri-implantitis).

Fig. 1
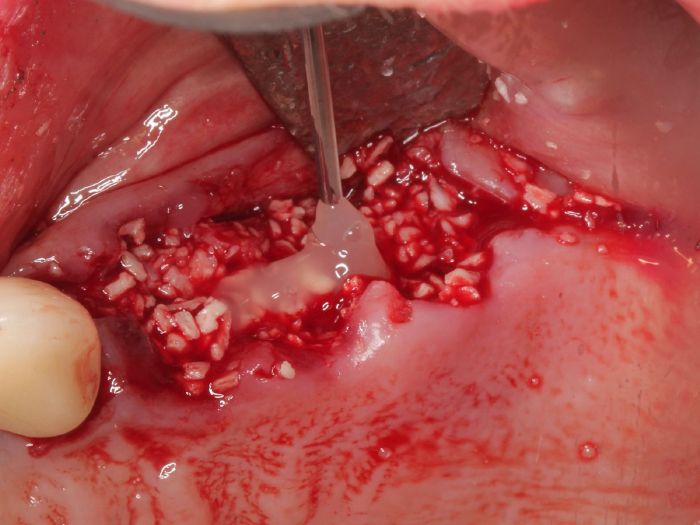
Fig. 2
Figs. 1 and 2 courtesy of Dr. Robert Miller (USA)

25 years of Straumann® Emdogain: How matrix proteins led to the breakthrough in regenerative periodontal therapy
Straumann® Emdogain® FL: Indications for the non-surgical procedure
- non-surgical periodontal therapy – pockets between 5-9 mm deep without furcations or recession involvement and
- in the curative flapless treatment of the early stage of peri-implant diseases (peri-implant mucositis).
here is a positive correlation between the use of the preparation and bone gain, implant survival and improved therapeutic success.2-4

Fig. 3
Emdogain®, Emdogain® FL and Labrida BioClean – our solution for peri-implant therapy
The best-documented material in regenerative periodontal therapy
“Emdogain® is currently the best-documented material in regenerative periodontal therapy and can be recommended for the treatment of intraosseous defects, grade II furcations and gingival recessions”, concludes Prof. Sculean in his webinar “Straumann® Emdogain® 25 years: Biological concepts for improved clinical outcome.”7 The closed procedure with Emdogain® FL is recommended for teeth with no furcation involvement, intraosseous bone defects and pocket probing depths of 5 to 9 mm.8th
Who invented Emdogain®? Hint: It all started in the 90s in a Swedish biotech lab…
Good preparation of the patient is crucial
An indispensable prerequisite for the success of a therapy with Emdogain® and Emdogain® FL as with any regenerative treatment, is good preparation of the patient: the tissue structures should be healthy and free of inflammation and the patient should be able to safely apply the techniques for optimal oral hygiene. There is now enough evidence that the rate of regeneration is comparable to that of membranes - only much easier for the dentist and less expensive for the patient. Due to the different dosage units (0.15, 0.3 and 0.7 milliliters), treatment with Emdogain® can be offered much more economically than with membranes. Depending on the morphology of the defect, for example if the extent of the defect is likely to result in the prepared flap collapsing into the bony defect, Emdogain® is used in combination with bone substitute material for support. In this way, the defect can be sufficiently stabilized and the soft tissue can be kept away from the defect.9

Emdogain® playlist on Youtube:
The use of Emdogain® in regenerative periodontal surgery
After the atraumatic incision, preparation and mobilization of the flap, Straumann® PrefGel®, 24% EDTA suspension (ethylenediaminetetraacetic acid) is applied to the cleaned root surface. After two minutes, it is carefully rinsed off with physiological saline solution, the surface is dried out and Emdogain® is immediately applied to the blood- and saliva-free root surface. In principle, recontamination of the conditioned root surfaces with blood or saliva during application must be avoided.

Fig. 4: Application of Emdogain® FL. (Picture courtesy of Dr. Min-Young Kim, Germany)
Stable suture closure
Another decisive factor for the success of the (surgical) therapy is stable suture closure. The wound must heal undisturbed. The flap is therefore fixed as close as possible to the neck of the tooth with atraumatic suture material. Postoperative complications and inflammatory reactions are extremely rare. There is no tooth cleaning in the operated area for at least three weeks and in the sulcus or approximal area for at least three to four weeks postoperatively (see Periodontal Treatment Guide, Straumann).10 In this phase, patients rinse with an antiseptic mouthwash (e.g., 0.1 to 0.2 percent chlorhexidine digluconate solution) or apply CHX gel locally for three weeks to prevent infection. An interdental brush may only be used in the operated area after six weeks at the earliest.