Initial situation
A 55-year-old woman was referred to our specialized periodontal office due to severe peri-implantitis combined with a general stage III grade b periodontitis (Fig. 1). The peri-implant disease had led to severe bone loss around two of three implants in the right mandible (Fig. 2). The patient was systemically healthy, but smoked 10 cigarettes per day. The peri-implant mucosa showed pocket probing depths up to 10 mm with bleeding on probing and suppuration.


Treatment Planning
The treatment was supposed to start with a systematic periodontal therapy including full mouth subgingival debridement accompanied by administration of systemic antibiotics. After reevaluation of the initial therapy following the first supportive periodontal therapy, the implants received another subgingival debridement combined with local antibiotics. After a healing period of about 2 weeks, the surgical intervention was planned as a combined regenerative-resective procedure with guided bone regeneration (GBR) and implantoplasty. After 8 months the result of the treatment should be evaluated.
Surgical procedure
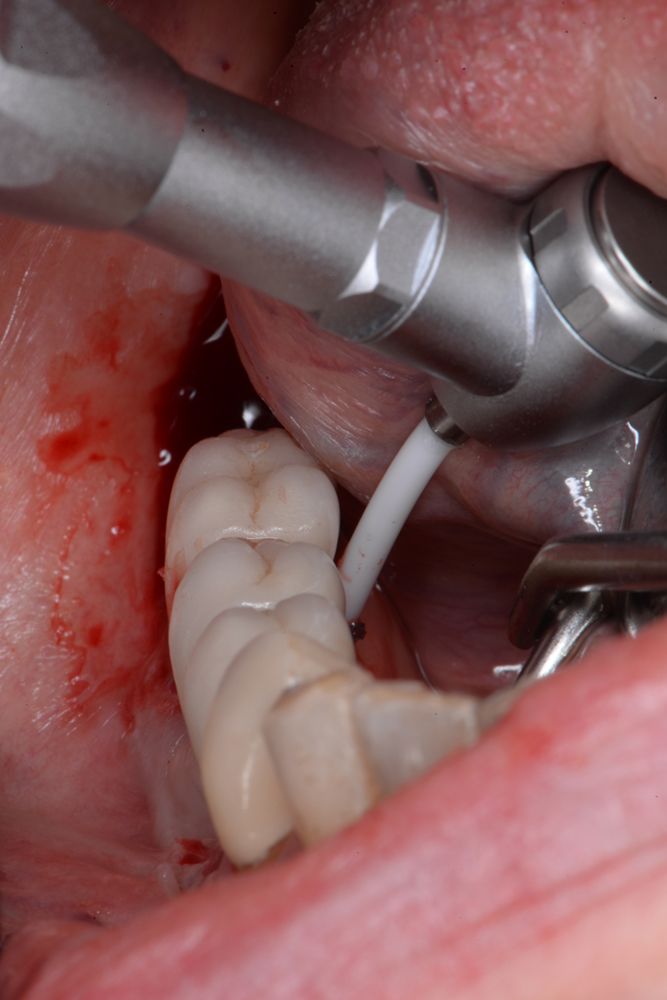
After periodontal examination, a full mouth subgingival debridement was performed following the principles described by Quirynen et al.1 and Cosyn et al.2. Amoxicillin 500 mg three times a day for seven days and Metronidazole 400 mg three times a day for seven days were administered as systemic antibiotics. After 8 weeks the reevaluation was performed with another complete periodontal examination and supragingival debridement. During the same treatment session, the area of the implants in the fourth quadrant was anesthetized and, again, a subgingival debridement was performed. During this procedure, a Labrida BioCleanTM chitosan brush was used to thoroughly clean the exposed implant surfaces (Figs. 3a-c).