Conventional and immediate loading with final n!ce® Screw-Retained Crowns with the Straumann chairside workflow
A clinical case report by Luis Cuadrado de Vicente, Cristina Cuadrado Canals, Andrea Sanchez Becerra, Luis Cuadrado Canals, Spain
Thanks to the extreme accuracy of modern intraoral scanners, excellent design software and reliable production systems, restoring an implant with a chairside model is now a reliable treatment with numerous advantages for the patient. The same day solution with final materials produces excellent implant crowns in a chairside environment.
Modern implantology is headed in the direction of the emerging concept of immediacy. This comprises different treatment protocols aimed at providing the patient with minimally invasive surgery and, where possible, a same day temporary restoration.
A reliable implant system, from the nanomolecular level to a complete restorative portfolio, is mandatory to provide this treatment. The core of the treatment is a full digital workflow, starting with optical impressions recorded with an intraoral scanner. To provide the same day treatments, the chairside model is mandatory. A digital intraoral impression and the corresponding design and production software and hardware enables the treatment team to obtain high-quality temporary or final restorations on the same day, without the use of a model.
The key elements of this immediate treatment are the implant placement, digital IO impressions, and the immediate design of the crown, which is then sent to a milling machine to produce the implant crown on a final, non-temporary, material. Pushing the boundaries of the “one abutment, one-time” concept, providing the final implant crown on the immediate loaded implant offers many advantages for the treatment team and the patient.
Accordingly, we present a clinical case where two different chairside approaches were applied.
On the upper maxilla, a conventional, delayed protocol was employed, and involved the placement of a Straumann® BLT implant, a two-month healing period and, finally, the recording of optical impressions with a 3Shape TRIOS3 IO scanner for the subsequent design and production of the final crown.
During the same treatment period, in the mandible, an immediate loading protocol was employed for a just placed Straumann® BLT implant. Optical impressions with the 3Shape TRIOS3 were also immediately recorded and sent to the computer with the chairside Trios Design Studio software to produce an immediate crown on a final material.
To provide this chairside model, the new Screw-Retained Crown module for Straumann® in 3Shape’s Design Studio software was used to design the implant crown on Straumann® Variobase®. This software provides the proven connection with the Straumann® CARES® C series chairside milling unit, allowing the design software to be connected directly to the CAM module of the C series.
CARES® C series is a robust and compact 4-axis wet milling and grinding equipment for in-house processing, especially designed to provide reliable and predictable precision when milling glass ceramics and hybrid materials. It comes equipped with intelligent 4-axis technology and improves the daily practice routine in terms of efficiency and productivity.
In this particular case, the new Straumann® n!ce® blocks were milled on the C series to obtain the final crowns. n!ce® material is a new high-tech, glass-ceramic solution that delivers fast, esthetic single tooth restorations. It can be milled, polished and seated, with no need for crystallization firing.
We selected a final material based on the case characteristics, with a minimally invasive approach, and provided the patient with a screw-retained crown on the same day to obtain excellent healing and shorten treatment time.
About Luis Cuadrado de Vicente

About Cristina Cuadrado Canals

About Andrea Sánchez

About Luis Cuadrado Canals

Related products and topics




Treatment planning
A Straumann® BLT Regular Neck, Roxolid®, Ø 4.1x12mm implant was placed at position #15. As insertion torque values and ISQ levels were not optimal for immediate loading, a delayed protocol with healing cap was selected.
Two months later, a panoramic x-ray showed an excellent situation for the BLT implant and correct healing of the #36 area (Fig. 1).
Following a chairside protocol, it was decided to load #15 and provide an implant treatment with immediate loading at #36 on the same day. This involved the design of two screw-retained crowns with the Trios Design Studio software, and their production in n!ce® material on the C series milling unit.

Fig. 1
Surgical procedure
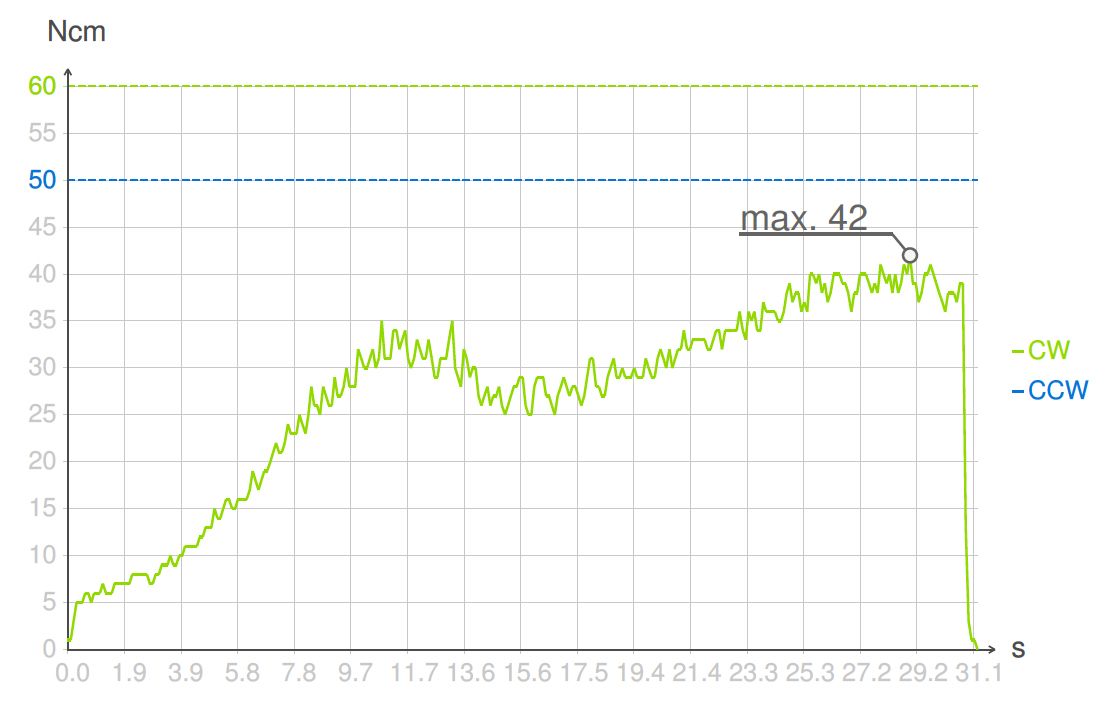
Under local anesthesia, a flapless implant surgery technique was performed at position #36. Due to the quality of the bone, staged drilling with continuous saline irrigation was performed in order to obtain a proper, safe insertion torque (Figs. 2-7). One implant (Straumann® BLT, Regular Neck, Roxolid®, Ø 4.8x10mm) was placed, and a torque of 42 Ncm was applied (Figs. 8-11).









The ISQ level was determined with the Osstell unit. After connecting the Type 54 Smartpeg, a score of 82 was obtained (Fig. 12). The decision to employ an immediate loading protocol has to take account of the surgeon’s personal experience and skills, insertion torque, ISQ levels and medical and dental characteristics of the patient. In this case, all these parameters were evaluated as excellent, and the immediate loading protocol was selected.

Fig. 12
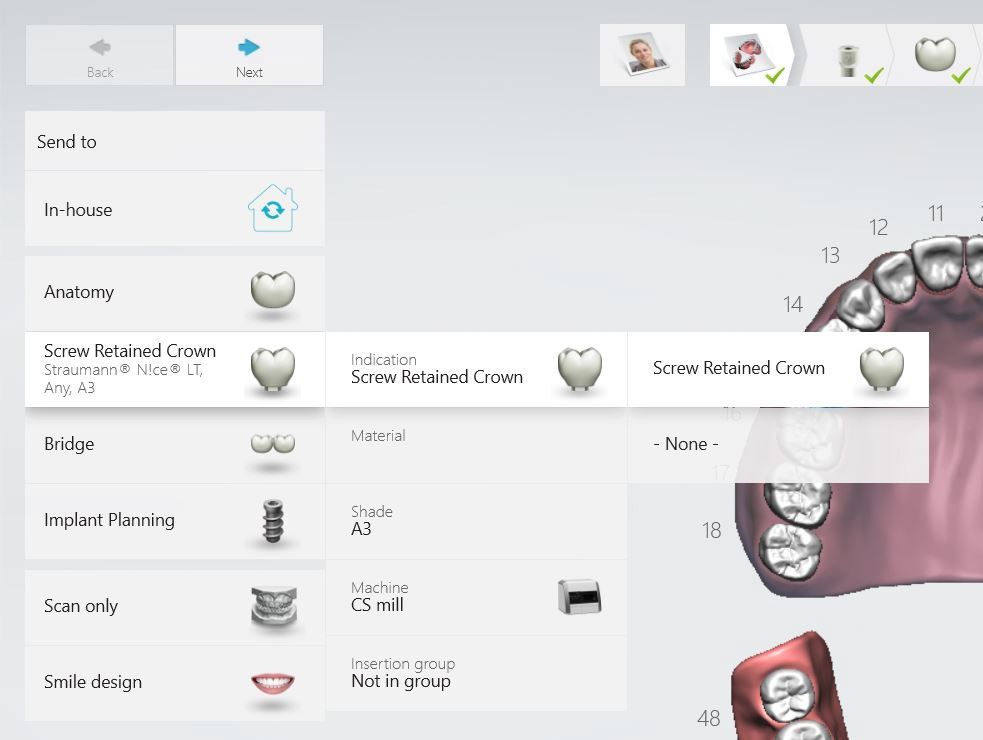
A Straumann® BLT scanbody was connected at implant level at both #15 and #36. An optical impression was obtained with the 3Shape TRIOS3 intraoral scanner after selecting the Screw-Retained Crown indication for Straumann® BLT implants on the Design Studio order form (Figs. 13,14).


Five scans were needed: lower jaw without the scanbody (emergence profile scan), lower jaw with the scanbody, upper jaw without the scanbody, upper jaw with the scanbody and, finally, the occlusion (Figs. 15-20).





During the prosthetic procedure, healing caps were placed to maintain the gingiva in position.
Prosthetic procedure
The SRC module of Trios Design Studio software is designed to be easy to use. Once the scanning steps are completed, the best fit between the virtual scanbody and the intraoral scanbody was determined using the three-point matching function, thus creating a digital model with the implant in its correct position (Figs. 21-22).


Once the alignment was approved, the next step was to use an auto-crown tool where the software created a suggested ideal crown. The software has different and excellent tools to shape and improve this initial auto-design (Figs. 23-24). After the crown is designed, the appropriate Variobase® is selected and the emergence profile designed. We chose the Straumann® RC H3.5 GH 1.0 Ti-Base (Figs. 25-27).





After the emergence profile design, a final sculpt step was done with automatic tools, adjusting the contact points and the occlusion in order to make the final adjustments to the full restoration (Figs. 28-29). The screw hole was established, and the crown was correctly placed and oriented in the virtual block (Figs. 30-31).




The computer was connected directly to the C series milling unit so that, after placing the n!ce® block in the holder, the milling of the crown could be started. After approximately 20 minutes, the crown was milled, including the screw hole and the connection to the Variobase® (Figs. 32-35).




Once the crown was ready, the selected Variobase® was cemented in the correct orientation in relation to the crowns. The crowns were stained and polished manually, and the whole process was finished about one hour after scanning (Figs. 36-39).




Returning to the patient, the healing caps were removed, and the crowns were placed. Occlusion was checked and contacts were inspected (Figs. 40-43). Screw holes were sealed with PTFE and a temporary filling material.




Treatment outcome
The patient and dentist were completely satisfied with the final result regarding esthetics, health and function. The overall treatment time per crown was about one hour from surgery to final crown delivery.
In this case the “same day crown” and “one abutment, one-time” concepts could be pushed to the limits in a simple and predictable manner thanks to a proven chairside workflow.
The patient returned for a check-up one week later and was very satisfied with the esthetic and functional outcomes of the treatment (Fig. 44).

Fig. 44