
Introduction
The following case report describes the interdisciplinary treatment of a medically compromised patient with a less invasive approach, avoiding a sinus lift procedure and using two short Straumann® BLX implants to restore a posterior edentulous area.
The Straumann® BLX implant is made of Roxolid® material and coated by a SLactive® surface. Roxolid® is a metal alloy composed of ~15 % zirconium and ~85 % titanium which is stronger than pure titanium and has excellent osseointegration and biocompatibility properties1-3. Moreover, the SLActive® surface has shown an extensive healing potential and recent studies have reported an outstanding clinical performance even in very challenging treatment protocols and patients with compromised health4-5.
In this case, these features played an important role to successfully treat this compromised patient and fulfill all his expectations in a very predictable way.
Initial situation
A 72-year-old male patient came to our dental practice with the chief complaint of poor masticatory function due to the loss of posterior teeth in the upper jaw. He referred that was looking for a fixed solution to replace the missing teeth in order to be able to chew properly.
His medical history revealed hypercholesterolemia and atrial fibrillation, which were under control with Atorvastatin (statin) and Edoxaban (anticoagulant). Moreover, he also referred a history of chronic periodontitis, which was the reason for his missing teeth.
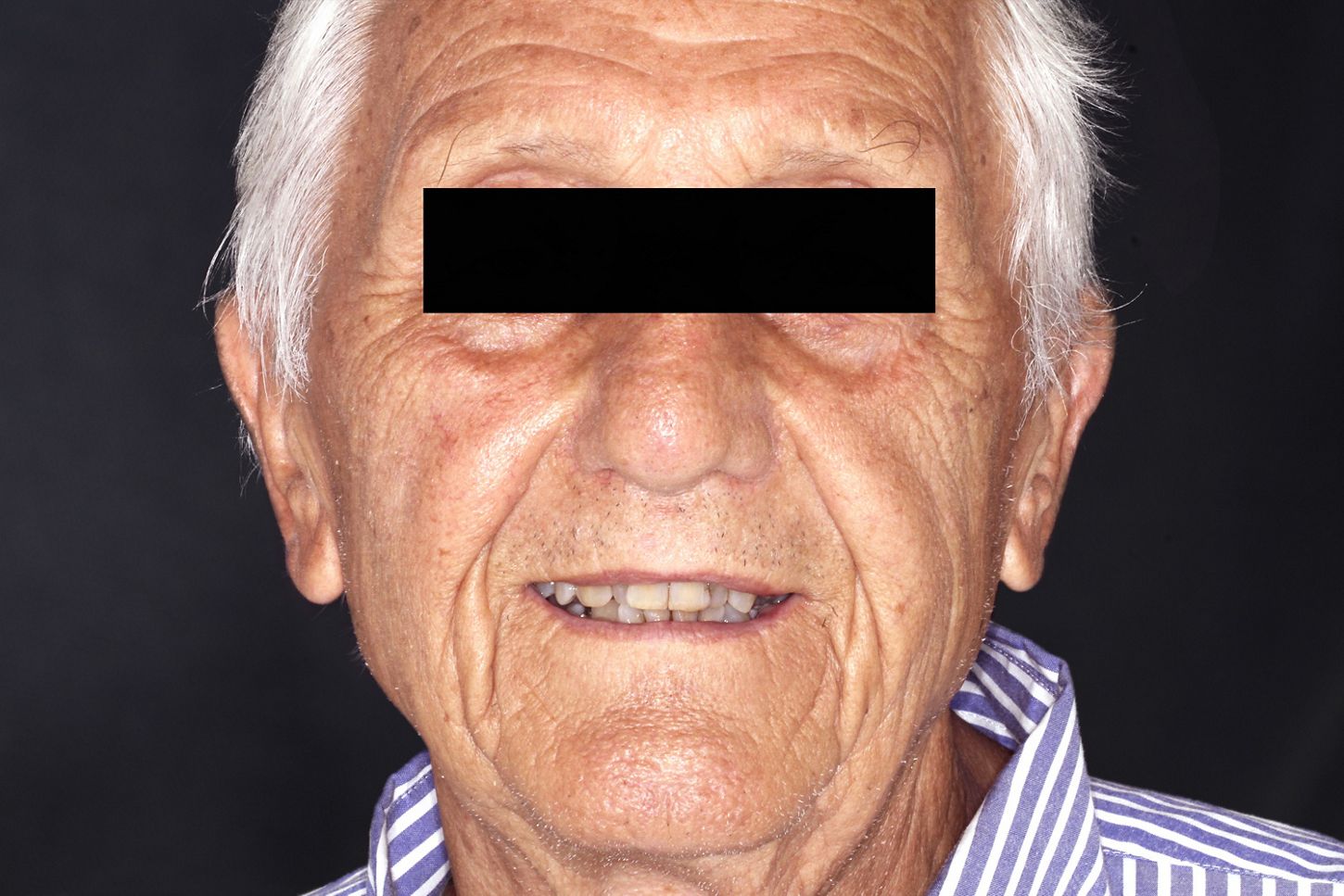
The extraoral examination showed a symmetrical and proportional face. The analysis of the smile demonstrated a midline sagittal plane coincident with the medium line of the smile, but with a lower midline 1mm deviated to the left side of the patient. Moreover, he presented a low smile line and the approximately exposure of the upper incisors and canines were 70% and 55% respectively (Figs. 1-3).


The intraoral evaluation revealed the missing posterior teeth on the left maxilla with a good amount of keratinized gingiva in the edentulous area (Figs. 4,5). Oral hygiene was evaluated as good.


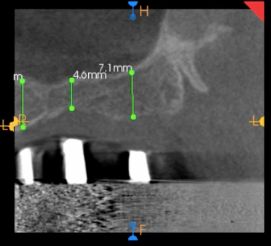
The radiographic evaluation was based on a panoramic radiograph and CBCT. The second quadrant displayed images compatible with absence of teeth #25, #26, #27 & #28, as well as limited vertical bone availability in this posterior maxilla area (Figs. 6,7).
The CBCT scan used radiopaque guides to facilitate the evaluation of the possible location of implants placed in positions #25, #26 and #27. Images compatible with thin cortical bone and very trabecular bone in this edentulous area were shown, as was the difficulty of placing a standard implant length due to the limited vertical bone availability (Fig. 7).

Treatment planning
Since his systemic condition required a team approach, before defining the treatment plan we asked for a consultation with his cardiologist. The specialist advised discontinuation of the medication one day before any surgical therapy and the avoidance of very invasive and prolonged procedures that could lead to extensive bleeding.
Following the systemic, clinical, and radiographic assessments, we were left with three possible treatment options:
- Open sinus lift with placement of two implants (immediate/delayed)
- Closed sinus lift with placement of two implants
- Placement of two fully tapered short implants
The selected treatment plan took into account the patient’s age, medical conditions and expectations. Taking these three points and the patient’s wishes into consideration, we decided to go for option number 3.
Many studies have shown short implants to be as predictable as standard implants 6-7, and this was one of the main reasons why we considered this option as the best for this patient, when bearing in mind a patient-centered solution with less invasive procedures. In this patient, the decision to use short implants was very important because it allowed us to perform a less invasive surgery. Performing a sinus lift procedure would have exposed us to an increased risk of postoperative bleeding.
Surgical procedure
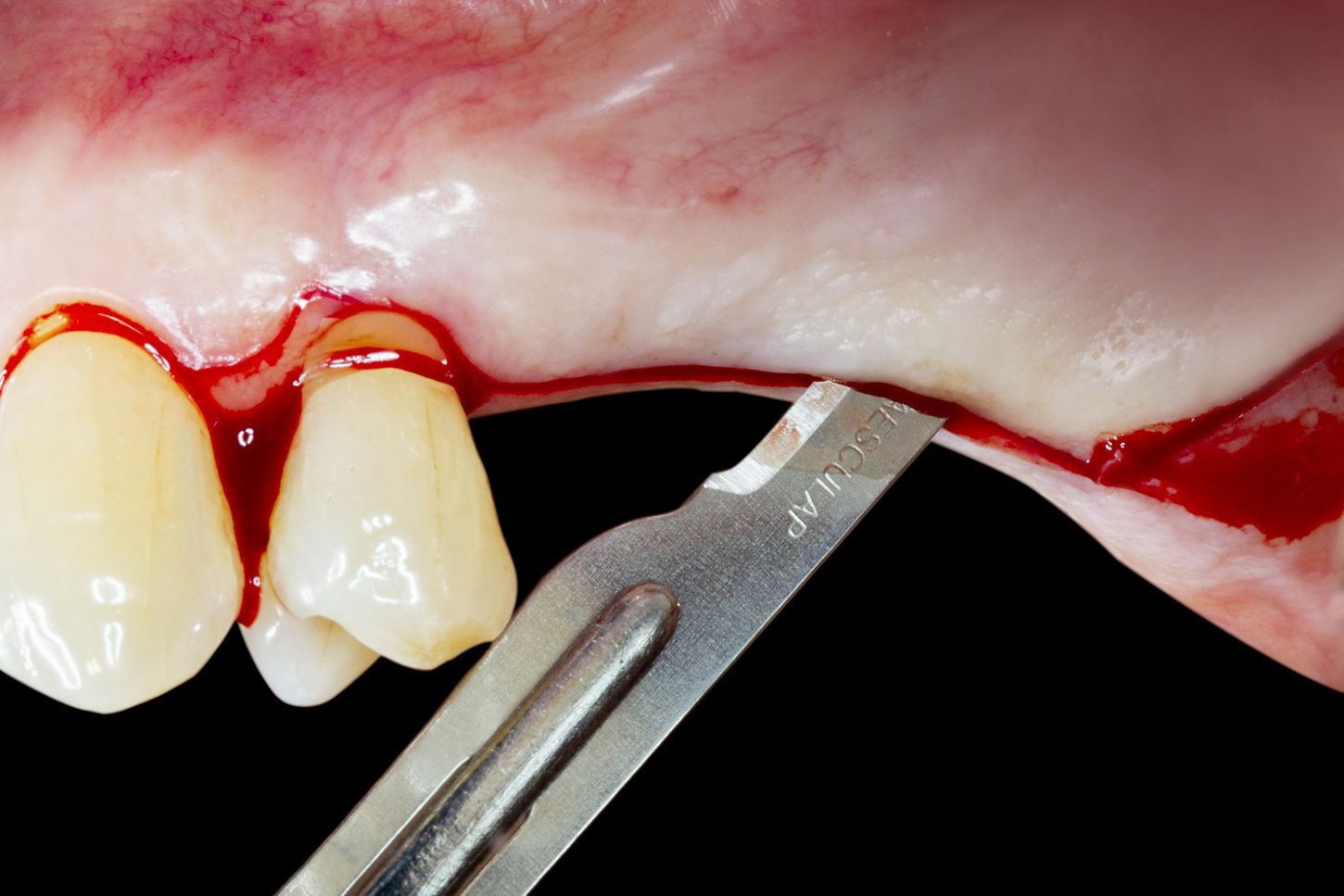
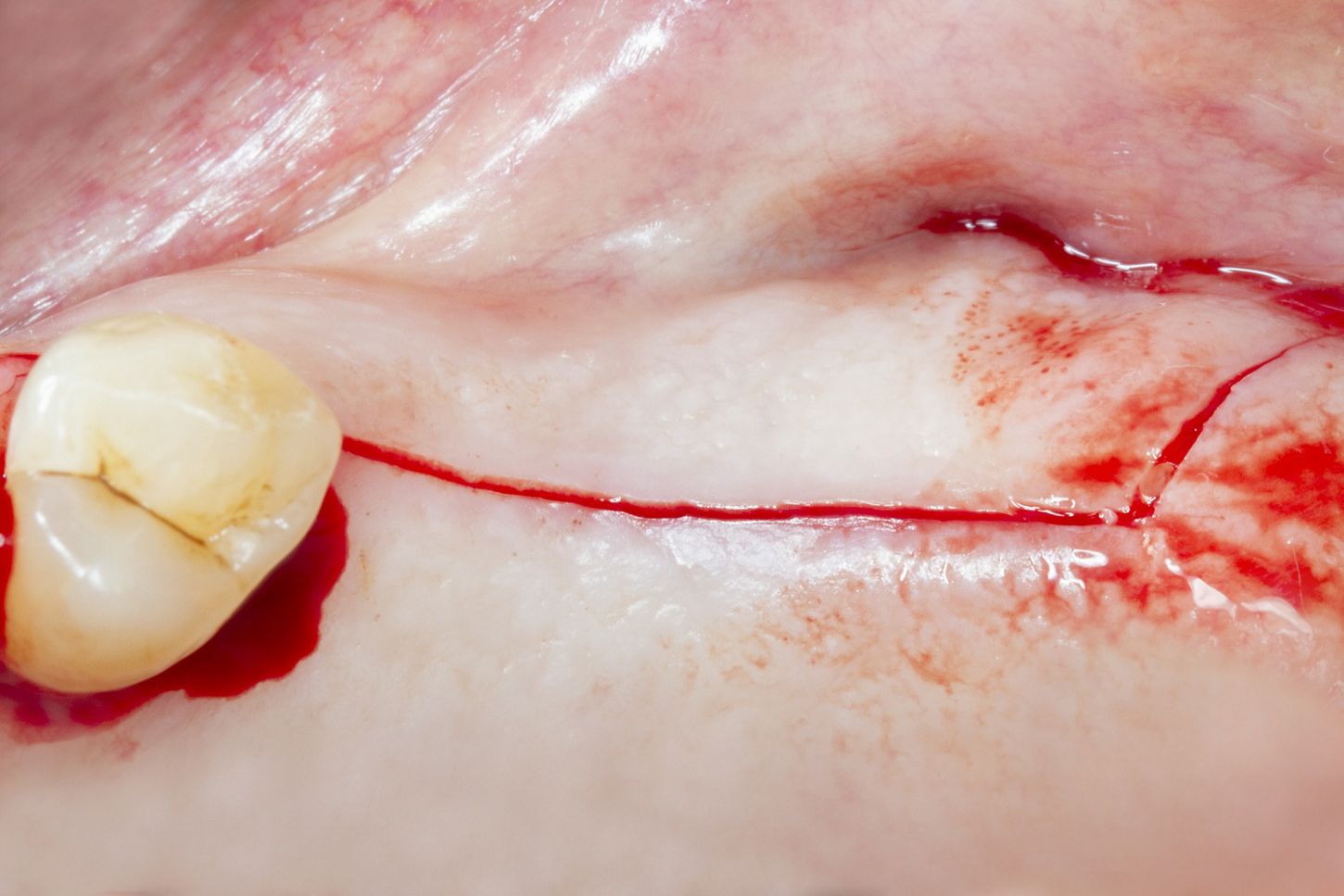
The patient underwent local infiltration anesthesia (lidocaine 2% with epinephrine 1:100.000), in the area corresponding to the apex of #25 and the molars of the second quadrant (Fig. 8). Intrasulcular, supracrestal, and distal releasing incisions were performed with a no. 15 blade (Figs. 9, 10).

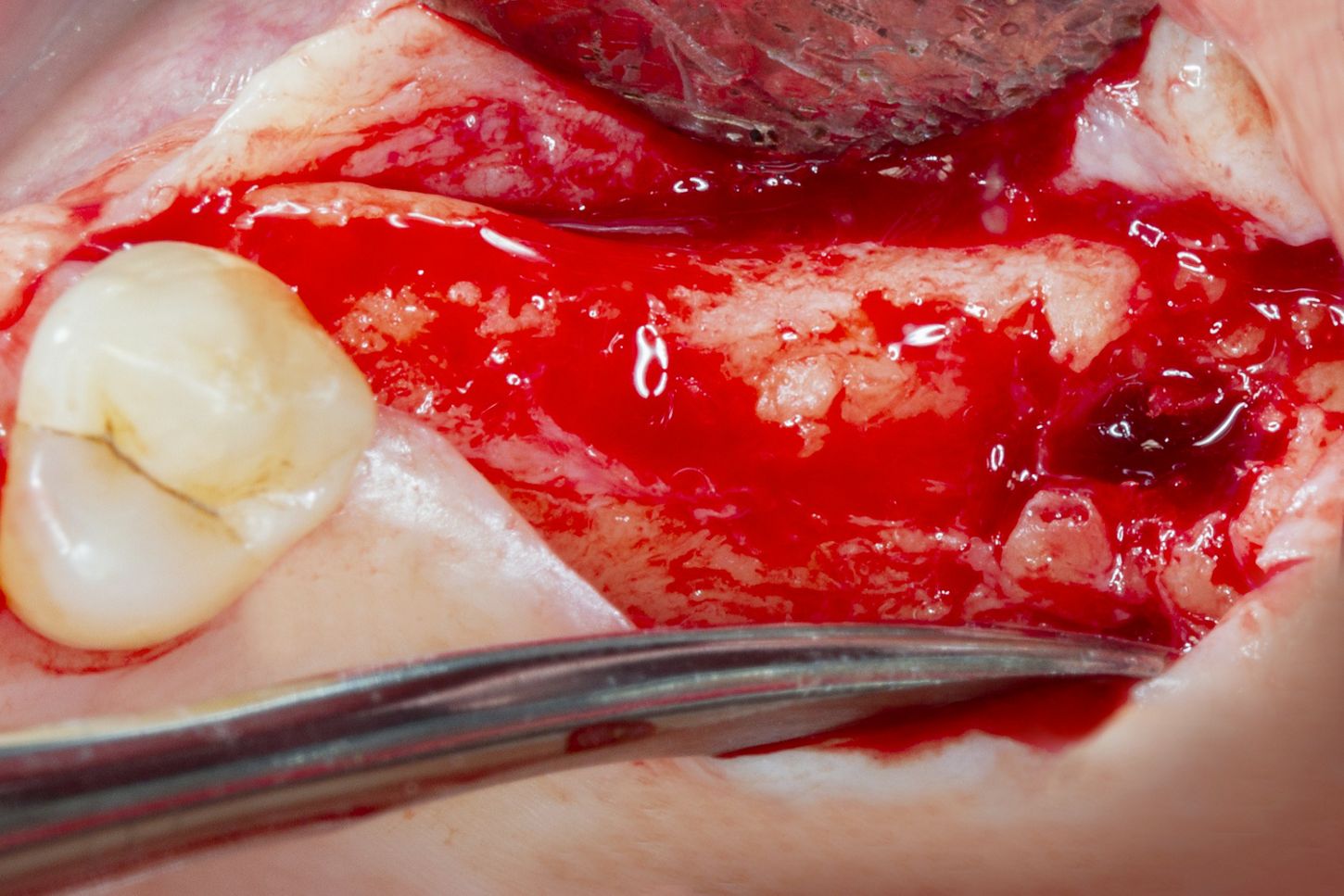
A full-thickness flap was then raised in order to gain access to the bone and evaluate the anatomy of the treated area (Fig. 11).
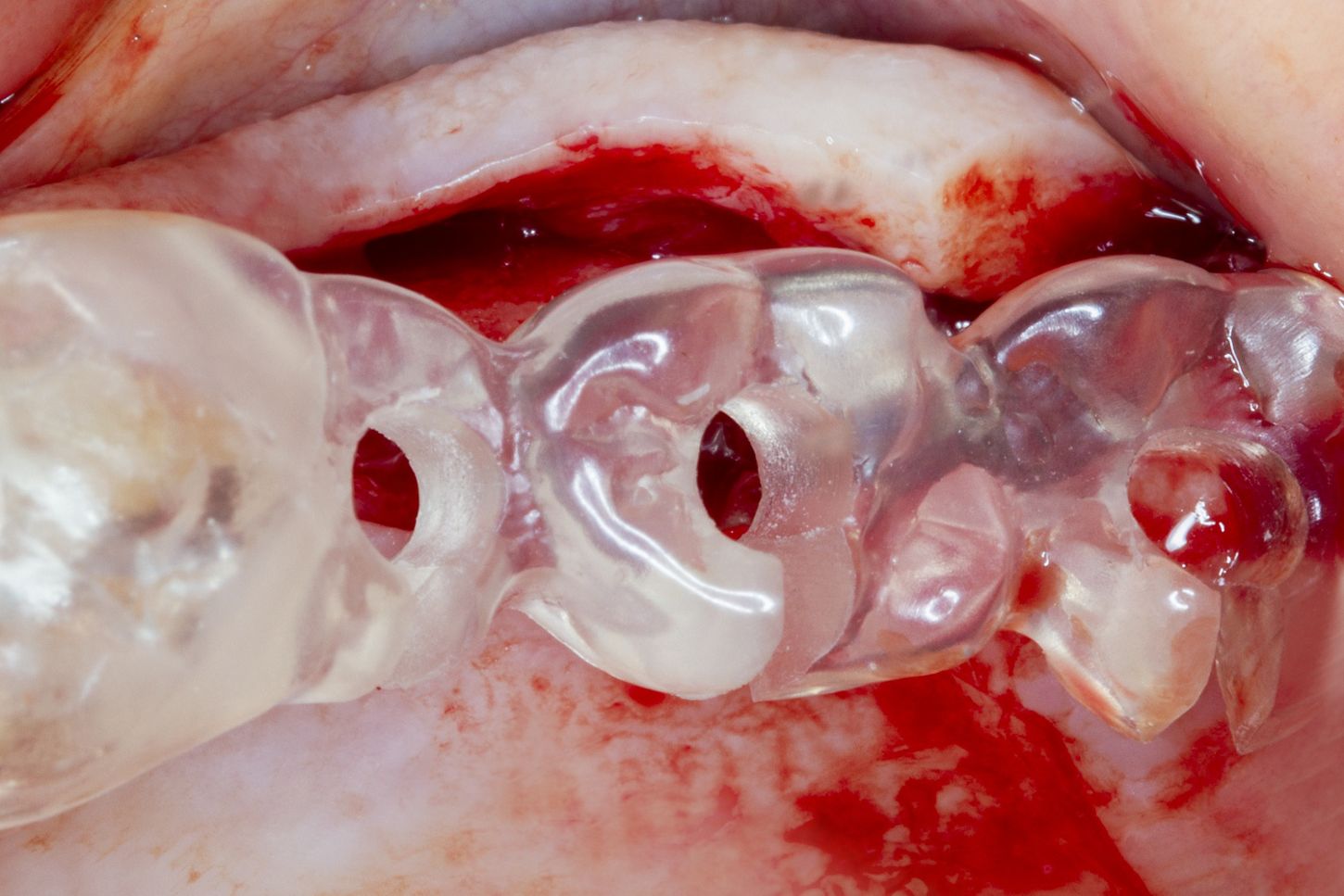
Based on the wax-up, a surgical stent was prepared in order to guide a prosthetically driven placement of the implants (Fig. 12). Following the flap elevation, the stability of this guide was verified (Fig. 13).
A medium quality bone protocol was followed to prepare the implant beds. Since we were placing a ø 4.5 mm implant, the ø 3.7 mm drill was the last one to be used.

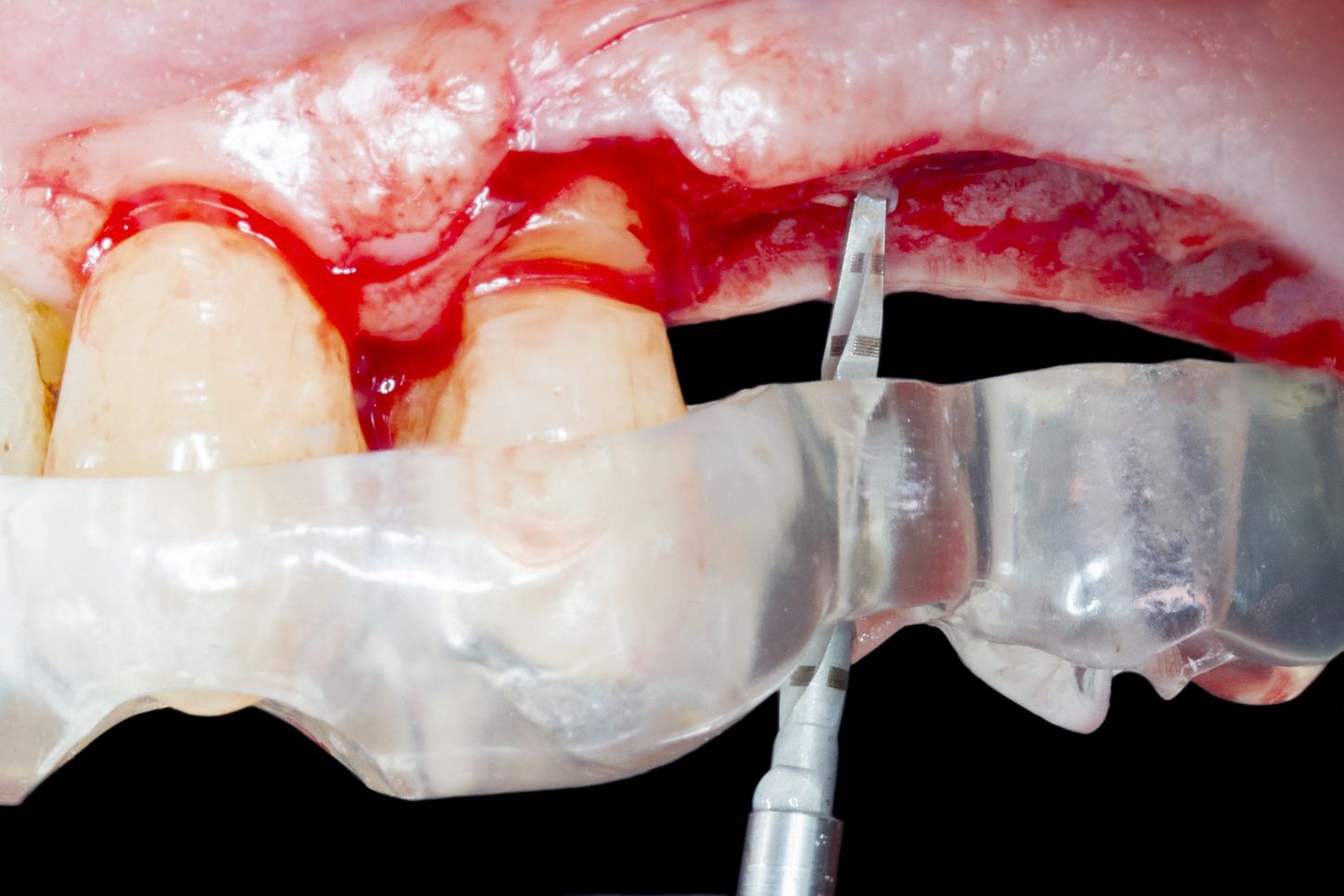
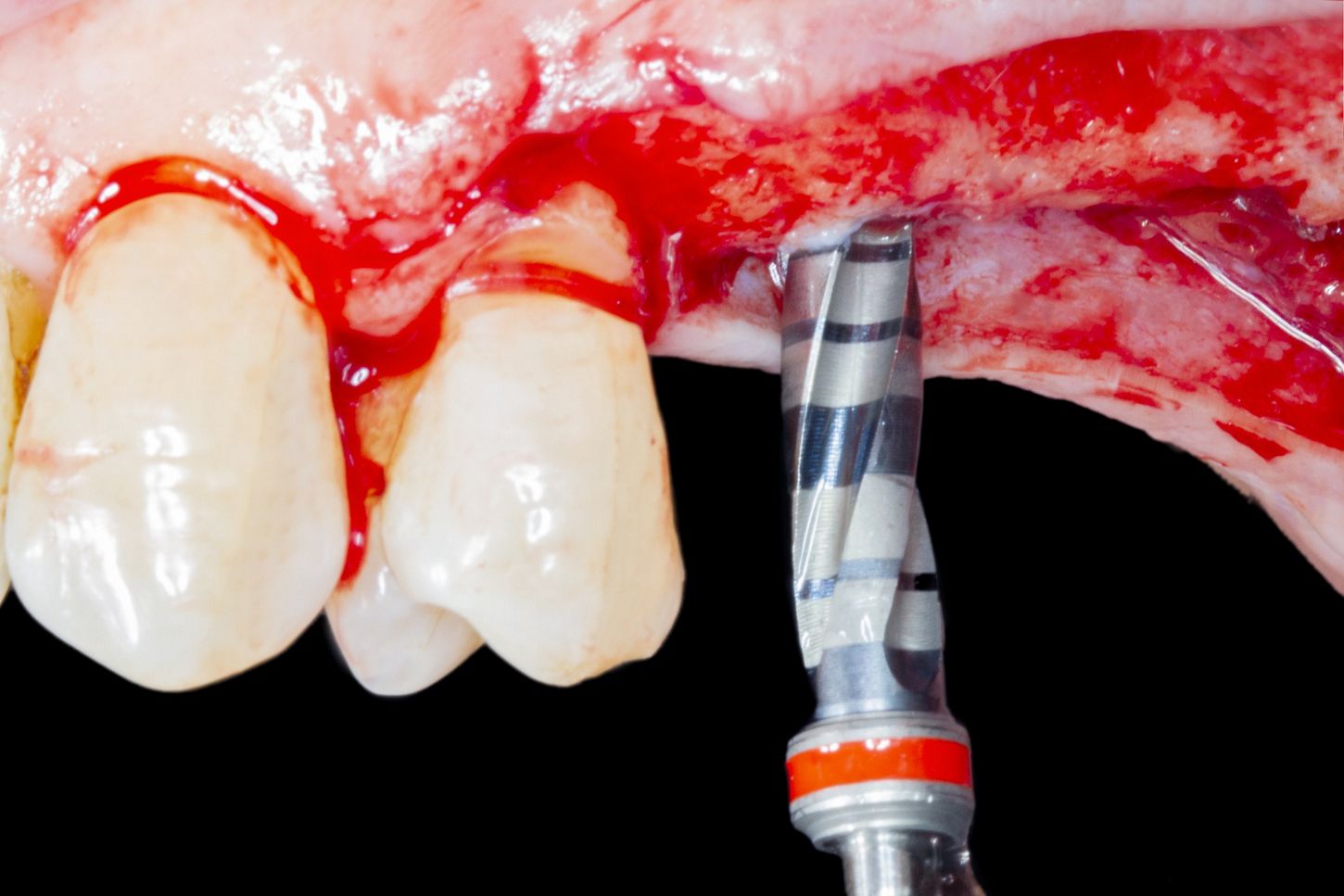
The drilling protocol started with the use of the needle drill (ø 1.6 mm), followed by the pilot drill/drill no. 1 (ø 2.2 mm), drill no. 2 (ø 2.8 mm), drill no. 3 (ø 3.2 mm), drill no. 4 (ø 3.5 mm) and, finally, drill no. 5 (ø 3.7 mm). Each drill was used under copious irrigation, and the tip was moved back and forth in order to avoid overheating (Figs. 14-19).




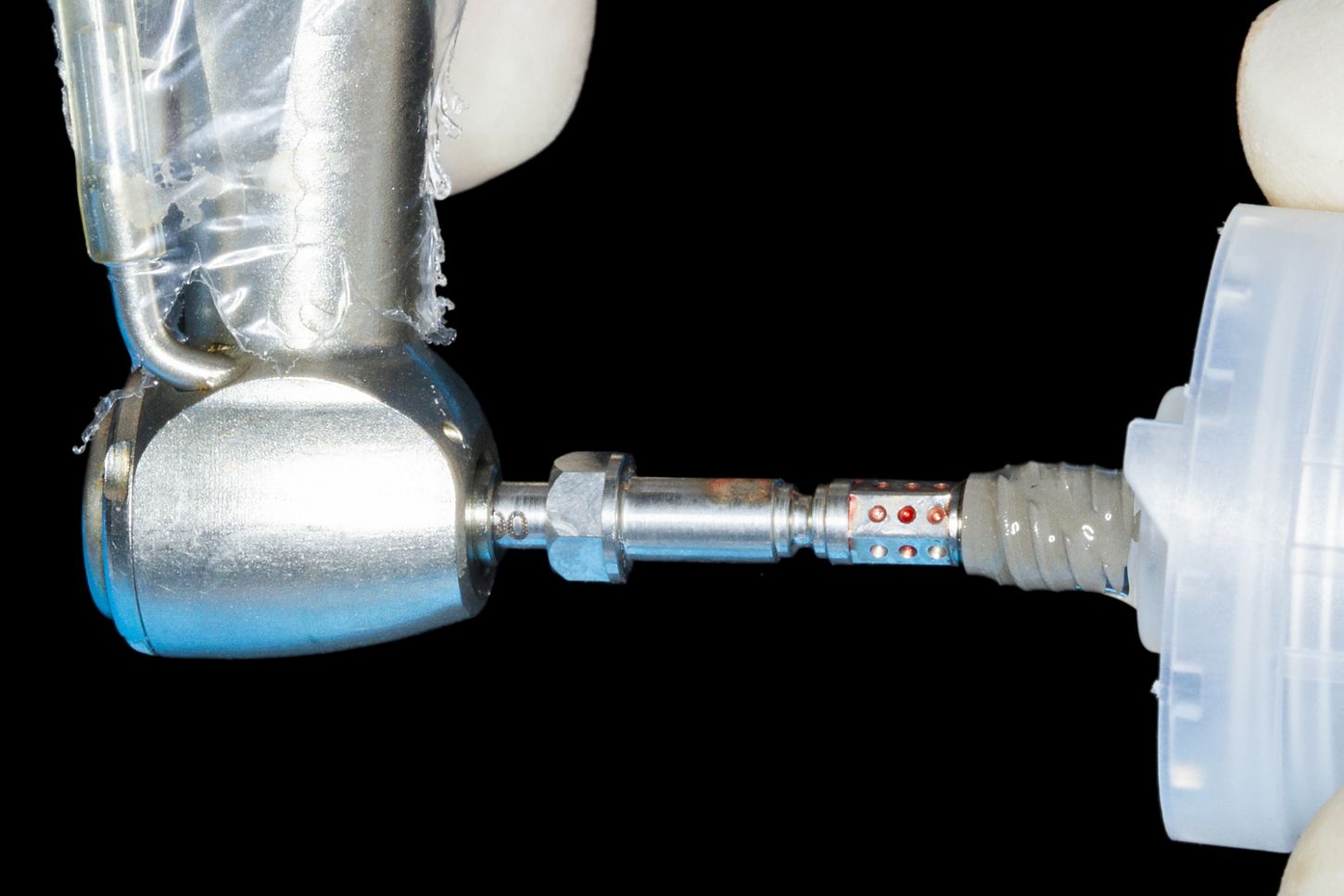
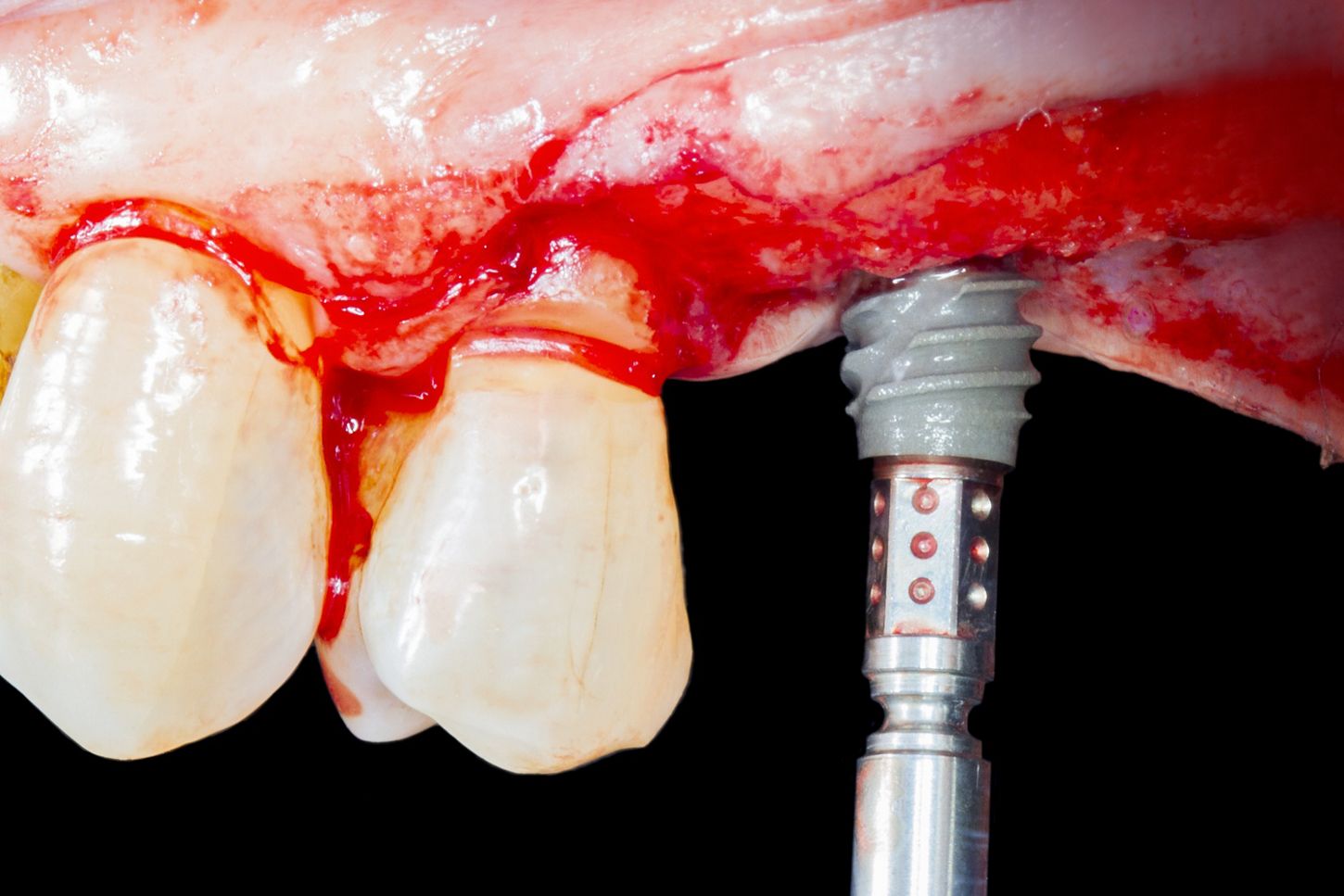
In accordance with the choice made during the treatment planning, a Straumann® BLX with 4.5 mm diameter and 6 mm length SLActive was used (Fig. 20). The implant was taken from the vial and removed with a slight clockwise turn (Fig. 21). Finally, it was placed on the prepared implant bed at position #25 (Fig. 22). The same procedure was applied for implant #27 (Fig. 23).


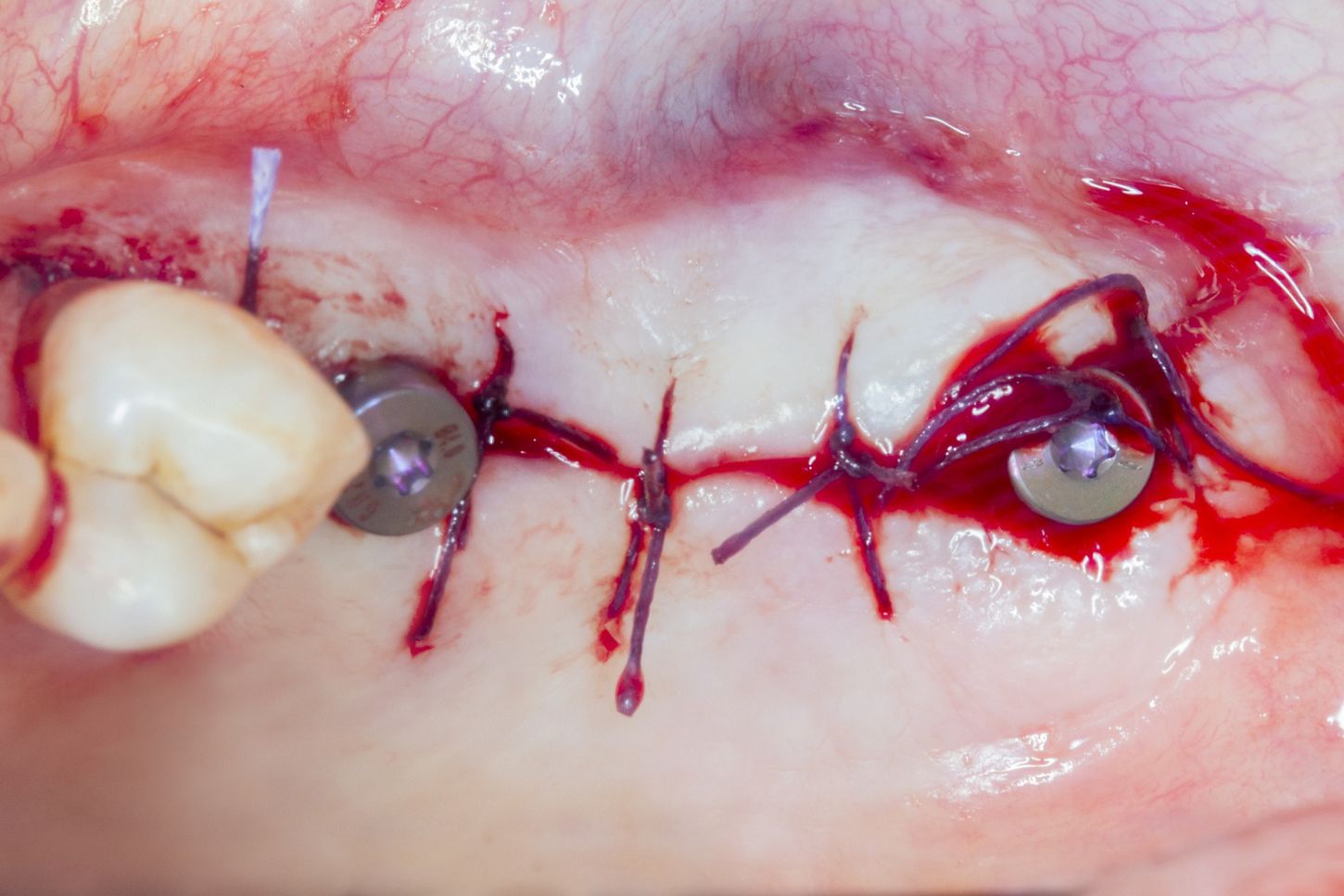
Next, both healing abutments were placed (GH 2.5 mm, ø 4.0 mm) and an optimal amount of buccal bone was observed on both implants (> 2 mm) (Fig. 24). Finally, the flaps were closed by the placement of interrupted sutures with Vicryl 5/0 (Fig. 25).

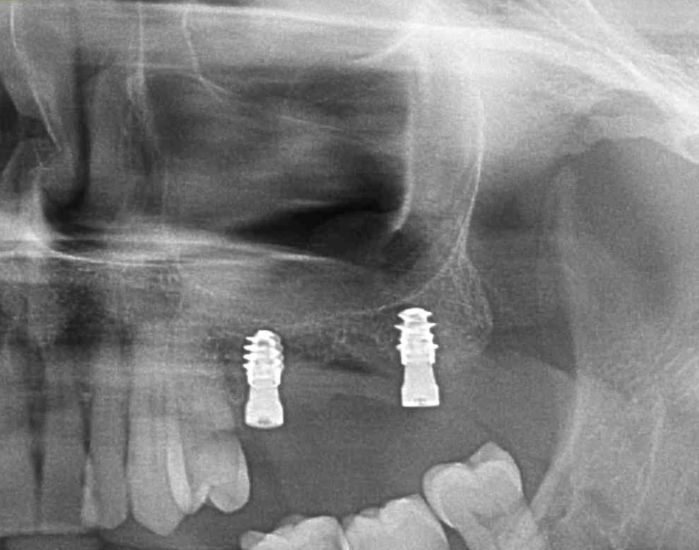
A postoperative radiograph showed an optimal vertical location of the two 6 mm implants. Furthermore, the maxillary sinus was not invaded, and both implants were in parallel alignment thanks to the drilling guide (Fig. 26).
After one week, the patient attended for a follow-up visit and the sutures were removed. The patient reported no pain nor complications and the healing was uneventful.
Prosthetic procedure
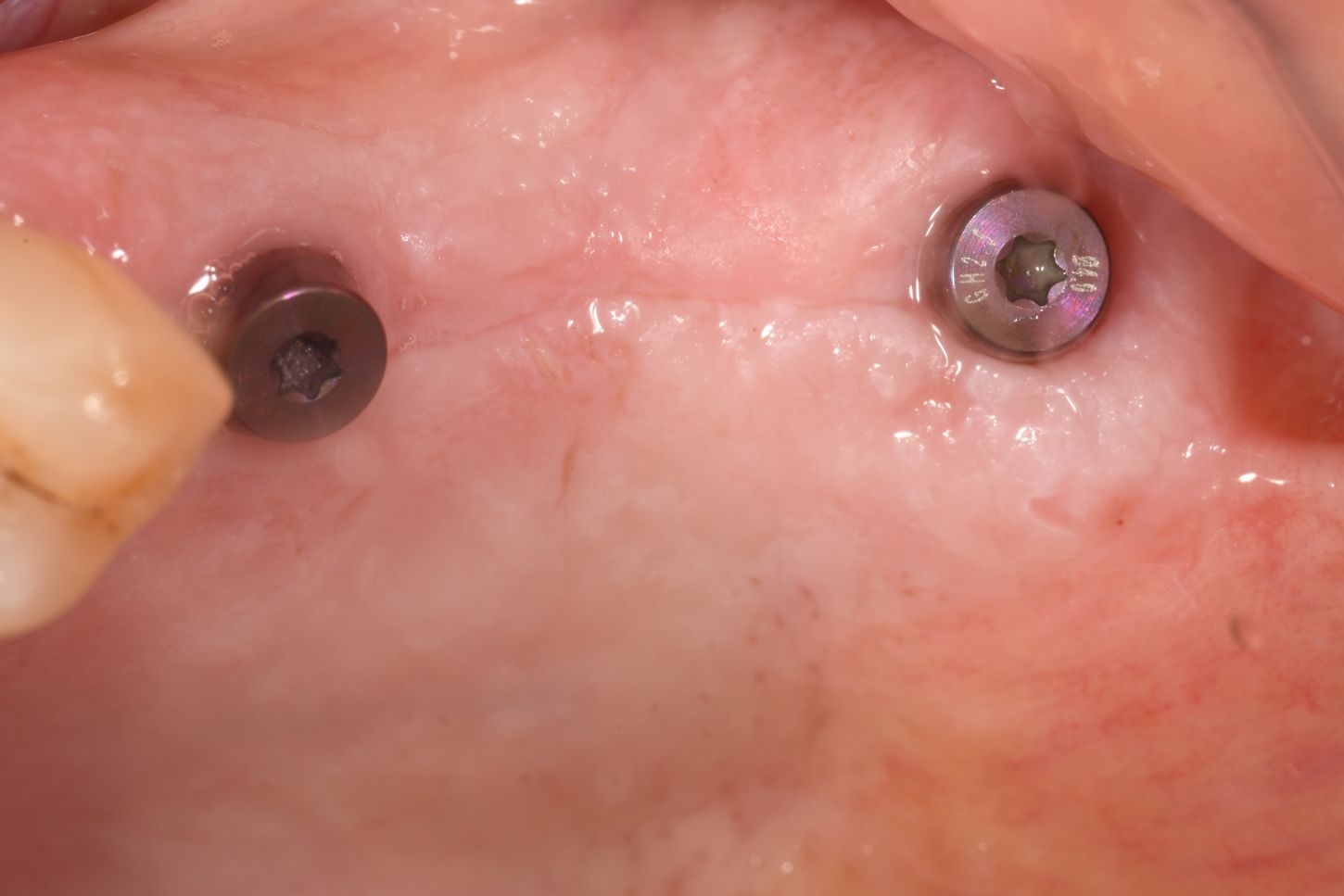
Four weeks after the surgery, the patient came back for the final impression and a complete soft tissue healing of the surgical site was observed (Fig. 27). Moreover, when removing the healing caps, we could appreciate optimal emergency profiles (Fig. 28).

Two scan bodies were screwed on top of the BLX implants and a 3Shape TRIOS® intraoral scanner was used to record the digital impressions (Fig. 29).

The data was then sent to the dental lab, where a screw-retained zirconia ceramic prosthesis was designed and produced using CAD/CAM. The color and design were selected based on the adjacent teeth, the patient’s own oral hygiene and expectations. Variobase® abutments were used (GH 1.5 mm ø 4.0 mm on implant #25 and GH 1.5 mm ø 4.0 mm on implant #27).
Finally, the final restoration was placed, and the patient was given detailed oral hygiene instructions (Figs. 30, 31).


Treatment outcomes
Medical and dental interdisciplinary cooperation is critical in the appropriate assessment of the medical history and the subsequent management of the medically compromised dental patient.
Thanks to the Straumann BLX implant design, material and surface, we were able to fulfill our patient’s expectations in a very predictable way.
The chosen treatment workflow proved to be the best option for this medically compromised patient. We obtained a good healing process, no postoperative bleeding complications, no morbidity and, consequently, a very satisfied patient who has now recovered his masticatory function.
Dr. Alfonso Caiazzo testimonial:
“My personal experience regarding the use of the 6 mm BLX implant has been extremely positive.
I found it to be a valuable tool when used on elderly patients, especially medically compromised ones, or in those for whom GBR is not advisable for various reasons, as major surgery is avoided in both cases. Furthermore, its design and surface are the perfect combination that allows me to perform surgeries even more rapidly and precisely. Additionally, with the SLActive® surface the loading protocol can usually be greatly shortened.
Despite the reduced length of the BLX 6 mm implant, I have reached very high insertion torques, even in soft bone and challenging clinical scenarios.”