Introduction
The ITI recommends immediate implant placement (type 1) in the presence of ideal anatomic conditions. This includes (i) a fully intact facial bone wall with a thick-wall phenotype (> 1 mm) at the extraction site, (ii) a thick gingival biotype, (iii) no acute infection at the extraction site, and (iv) a sufficient volume of bone apical and palatal to the socket to allow implant insertion in a correct 3D position with sufficient primary stability. When these ideal conditions are not met, it is suggested to place implants after 4-8 weeks of soft tissue healing (type 2). If primary stability cannot be achieved after 4-8 weeks, the post-extraction healing period should be extended to allow for partial bone healing (type 3).1 Type 4 is the placement of the implant into a fully healed site.2
An adequate amount of bone is needed to be able to place the implant in an ideal prosthetic-driven position. If there adequate bone volume is not available, guided bone regeneration (GBR) techniques should be used for ridge augmentation before implant placement.3
The following case report describes an interdisciplinary treatment that included orthodontic therapy, guided bone regeneration (GBR), implant placement, and fixed restorations. Ceramic braces were used to level, align, and gain space for implant placement at a central incisor location. Because of the complexity of this clinical case, the GBR was first carried out with a non-resorbable membrane and Cerabone® and, after six months, a Straumann® BLX implant was placed.
Initial situation
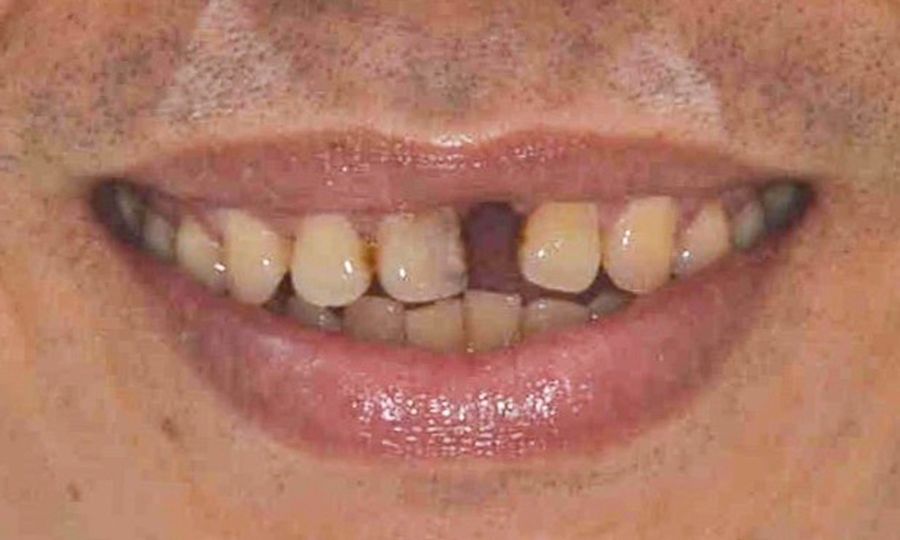
A systemically healthy 48-year-old male patient came to our clinic seeking an esthetic and functional treatment for a missing anterior tooth. He reported being a non-smoker, taking no medication, and with no allergies. His chief complaint was, “I feel very embarrassed to talk and smile in public because I have a missing tooth. I would like to have a fixed restoration and a nice smile. I don’t want to wear this denture any longer.” His dental history revealed the loss of tooth #21 during an accident over 20 years ago. Since then, he had noticed that the space left by the central incisor was slowly being closed by the adjacent teeth. The extraoral examination revealed a medium smile line with an impaired mesiodistal (MD) proportion of the anterior teeth. Due to the limited MD availability on position #21, the provisional restoration looked small and narrow. Moreover, the anterior teeth were not level, resulting in a reverse smile. For the intraoral examination, the provisional denture was removed. Neighboring teeth were mesially tilted (Fig. 1).
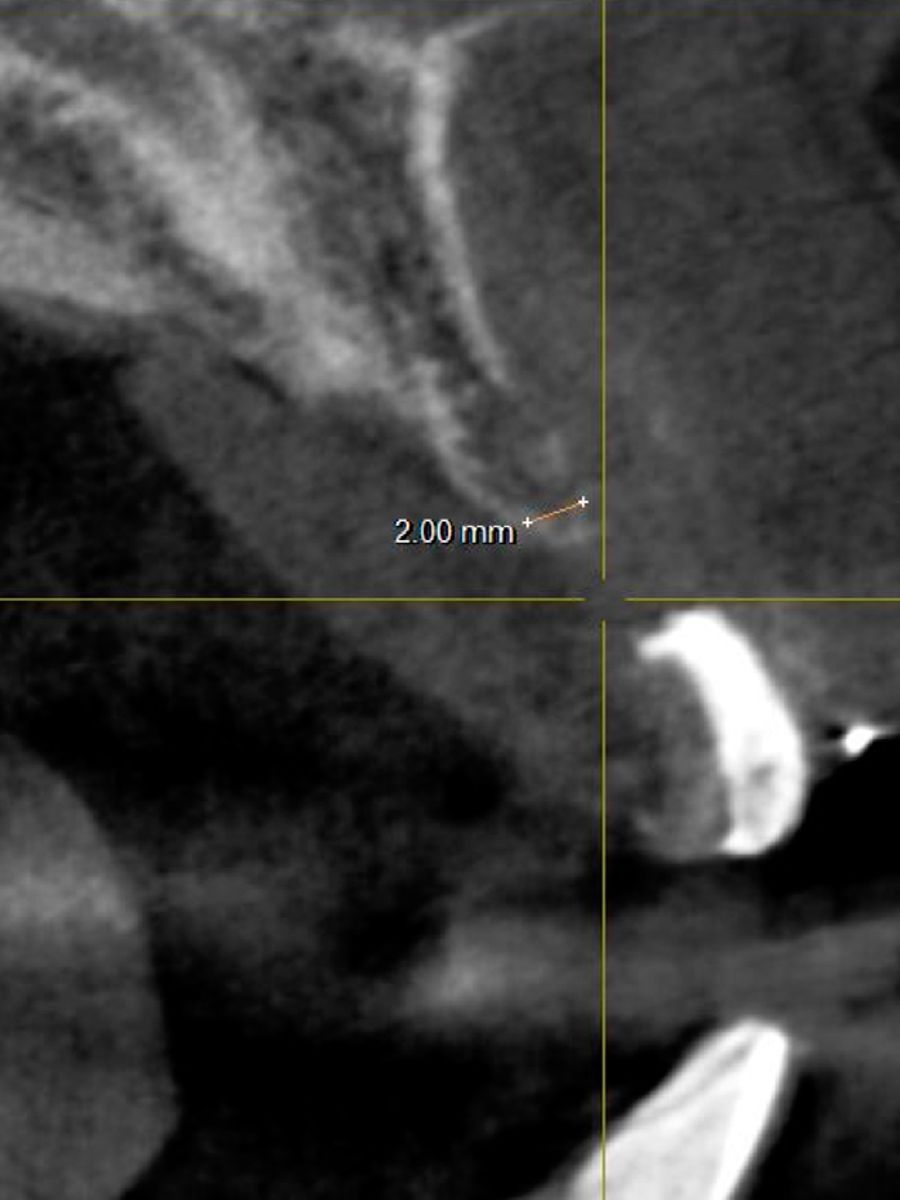
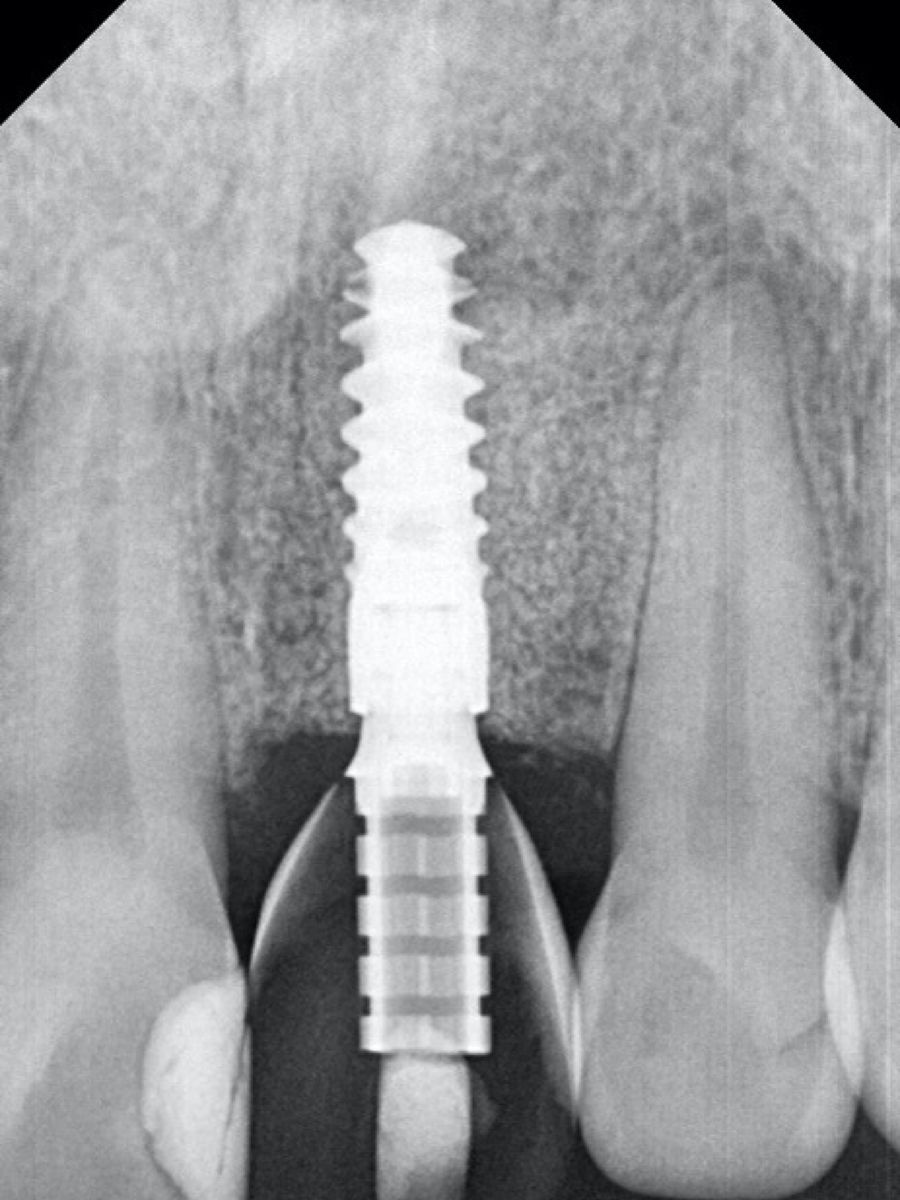
Since the residual ridge was atrophic, a severe horizontal ridge defect was apparent, and secondary caries was present in #11 distally (Figs. 2-4).