Contemporary research estimates a prevalence of 22%2; and as the global number of patients treated with dental implants increases, peri-implantitis is considered to be a major challenge in dentistry. Thus, prevention and appropriate management of this condition are becoming increasingly important for the general dentist and specialist.
The appropriate treatment protocol depends on proper diagnosis and should be tailored to the severity of the lesion and the patient’s risk factors. Depending on disease progression, the clinician needs to decide if the treatment goal is to arrest disease progression, regenerate the tissues or explant and replace the dental implant.
The following case report describes the treatment of a patient diagnosed with peri-implantitis in an upper premolar site, with advanced bone loss. The failed implant was removed with conservative techniques, avoiding damage to neighboring structures and preserving as much bone as possible. The implant was replaced with a Straumann® BLX Roxolid® SLActive® implant and the tissues were reconstructed using bone granules (maxgraft®, botiss, distributed by Straumann Biomaterials) in conjunction with a collagen membrane (Jason®, botiss, distributed by Straumann Biomaterials).
Initial situation
A non-smoker 75-year-old female patient presented to our clinic with the chief complaint of pain and discomfort in the upper right maxilla. A dental implant had been placed 3 years ago in position #14.
Her medical history revealed heart surgery 15 years ago, where a coronary stent was placed to avoid coronary artery obstruction. Following the cardiovascular surgery, her cardiologist prescribed acetylsalicylic acid (100 mg/day) and a drug based on the active ingredient ramipril (2.5 mg/day). She was also prescribed rosuvastatin (5 mg/day), a statin to treat hypercholesterolemia and prevent further cardiovascular complications, and was advised to eat a healthy diet and exercise.
She also reports that she has been taking an anxiolytic (trazodone, 50 mg/day for the past 5 years since the death of her husband.
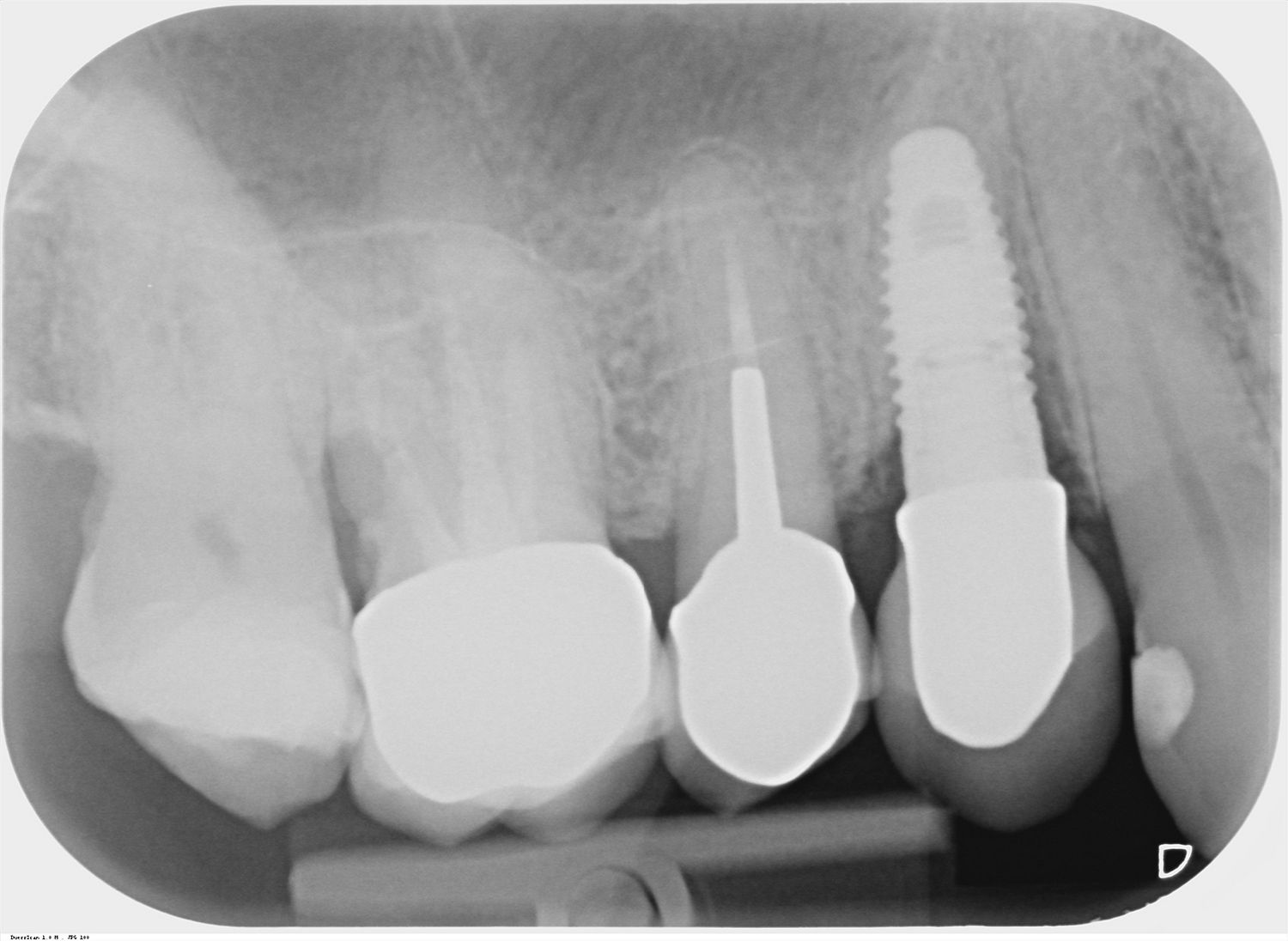
The intraoral examination revealed erythematous buccal mucosa, 9 mm probing pocket depth with bleeding on probing, and a vestibular abscess in the region of implant #14. Her oral hygiene was evaluated as good.
The radiographic evaluation showed moderate interproximal vertical and horizontal bone loss (Fig. 1).