Initial situation
A 70-year-old female patient presented to our practice with an unstable and non-esthetic tooth-supported two-unit bridge. Her chief complain was to recover the function and aesthetics in this posterior area. Additionally, she had very high expectations in regard to the predictability of the treatment and highlighted her wish of a long-term solution, independently of the price.
Her medical history reveled an adenocarcinoma (breast tumor) which was treated 20 years ago and pharmacological controlled cardiovascular diseases with beta-blockers and acetylsalicylic acid. Given her systemic condition, the patient was derived to her cardiologist for an evaluation prior the start of the preparation of the treatment plan.
The positive feedback from the specialist allowed us to continue with the treatment, including surgical procedures and without interfering with the patient’s medication.
The clinical evaluation of the third quadrant showed a tooth-supported two-unit bridge (#34- #37) with apparent signs of unaesthetic coating fracture, breakage of the underlaying metal, infiltration of the underlying abutments and mobility; which indicated the need of a new restoration, evaluation of the abutments and assessment of the edentulous area (Fig. 1).

In order to do a better assessment and evaluate the abutments, it was decided to remove the bridge prior the x-rays procedures.
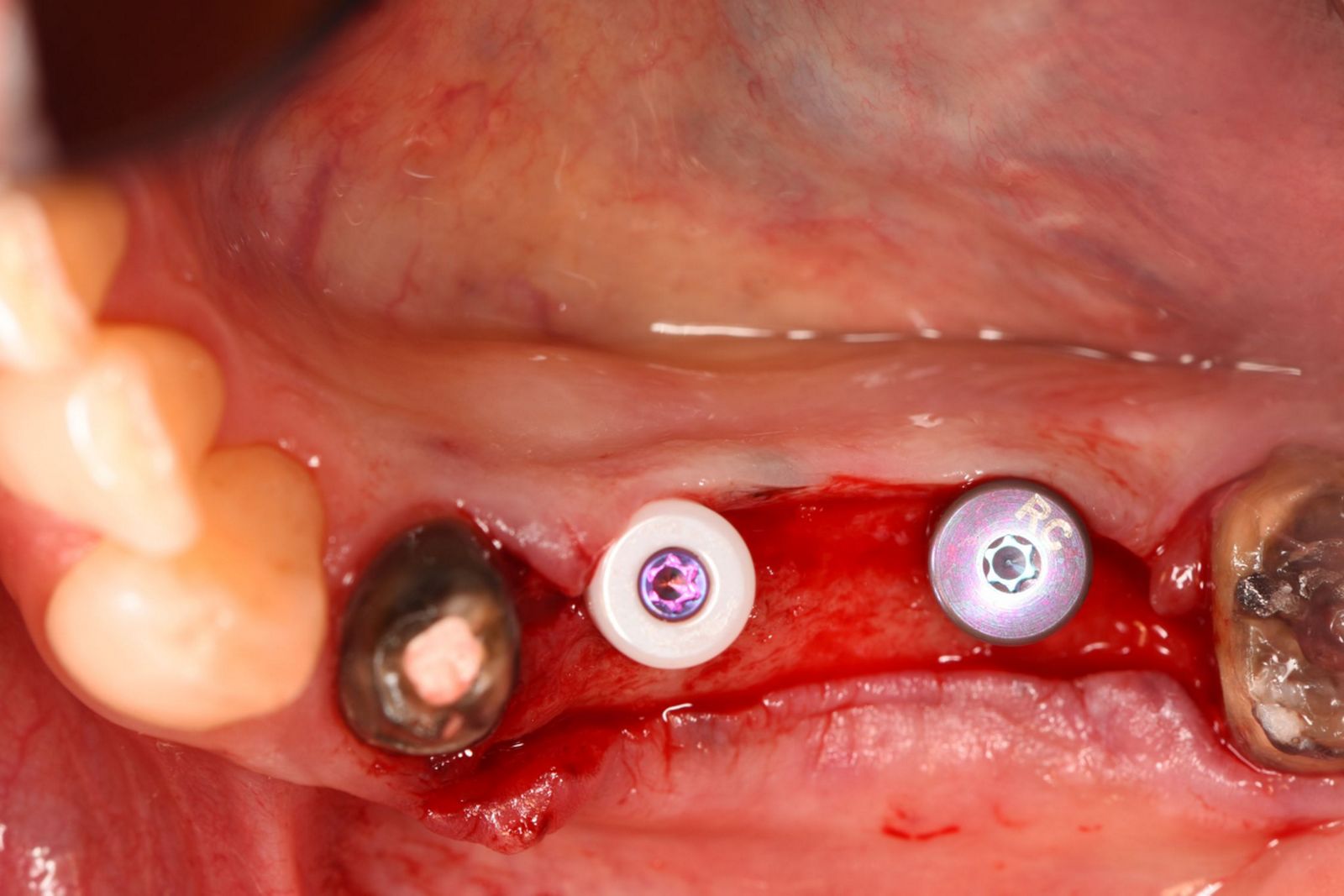
The clinical evaluation of the abutments showed a limited amount of keratinized tissue in the premolar region, a regular shape of the edentulous ridge and an acceptable horizontal width. Moreover, an amalgam tattoo was also appreciated on the supracrestal area of position #35 (Fig. 2).

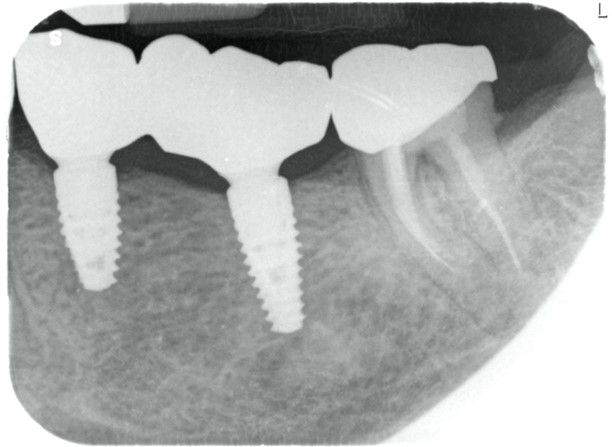
The radiographic evaluation showed images compatible with periodontal ligament widening, root canal treatments and periapical lesions on teeth #34 and #37. Furthermore, vertical bone availability was observed (Fig. 3).