
Tooth replacement by implant in patients with thin gingival tissue generates concern due to gingival translucency, where the greyish colour of titanium may result in aesthetic failure of the treatment. In this respect, zirconia implants differ mainly because of their light colour, which is close to the colour of the root, and because of their biocompatibility. They also allow the patient to opt for entirely metal-free treatment. The report on this clinical case demonstrates a technical innovation using a zirconia implant to resolve an aesthetically highly complex clinical case in a young patient with thin gingival phenotype and a high level of aesthetic requirements. The case was completed with a cement-retained prosthesis and metal-free crowns made using injection-molded ceramic. After completion of the case and follow-ups for one year, it was concluded that, despite the technique sensitivity, the zirconia implant enabled resolution of the aesthetic issues in this clinical case of thin gingival phenotype without the use of gingival grafts.
Introduction
Nowadays, patients are increasingly concerned with the aesthetic resolution of dental treatment, seeking a smile in which the implant cannot be seen. In this sense, cases that require replacement of only one tooth and have no other aesthetic interferences in adjacent teeth or in the gingival tissue are highly relevant1-3.Since the description of osseointegration by Branemark et al. (1977)4, implants have traditionally been made using commercially pure titanium or alloys containing titanium, offering high biocompatibity and mechanical resistance5. However, in the search for treatment of a high aesthetic standard, mainly in young patients with thin gingival phenotype where there are concerns over gingival translucency, the grey colour of titanium may lead to treatment failure6-8. In order to resolve discolouration of the gingival margin, prosthetic ceramic components were created9. However, these components still have a metal strip at the bottom and, since they are hybrid pieces, are more likely to break or come loose from the metal body10. In this respect, zirconia implants differ mainly because they are normally made in one piece, which increases their mechanical resistance. Their light colour mimics the colour of the root and they are biocompatible. They also allow the patient to opt for totally metal-free treatment11-13. Another advantage of zirconia is its low affinity for bacterial biofilm, which reduces the risk of gingival inflammation. Concerning osseointegration, treating the surface of the zirconia implant with blasting followed by acid conditioning (ZLA® surface) provides an osseointegration capacity comparable to titanium implants treated in the same way13,14. The choice of a zirconia implant has thus become plausible, particularly in young patients, who normally have a white aesthetic with no interference from other prostheses, restorations or gingival recessions. They are seeking a solution that will be imperceptible in relation to their other teeth. Therefore, this clinical case report exemplifies the use of an innovative zirconia implant for a highly complex aesthetic solution in a young patient with thin gingival phenotype.
Clinical case report
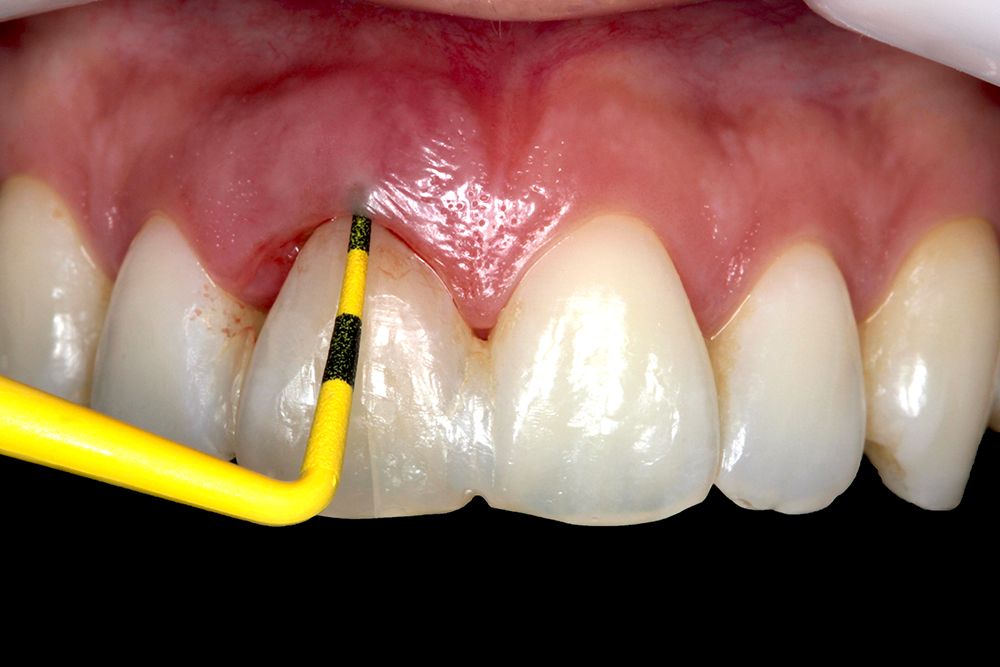
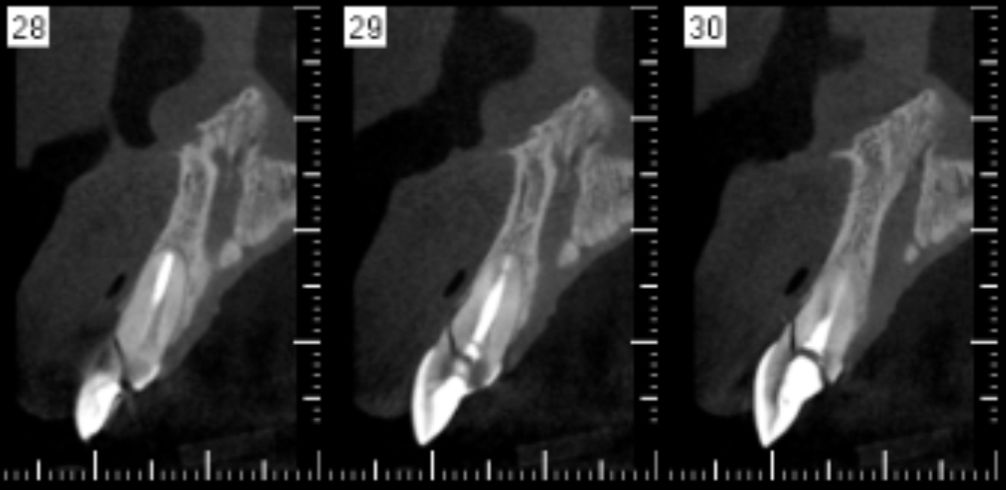
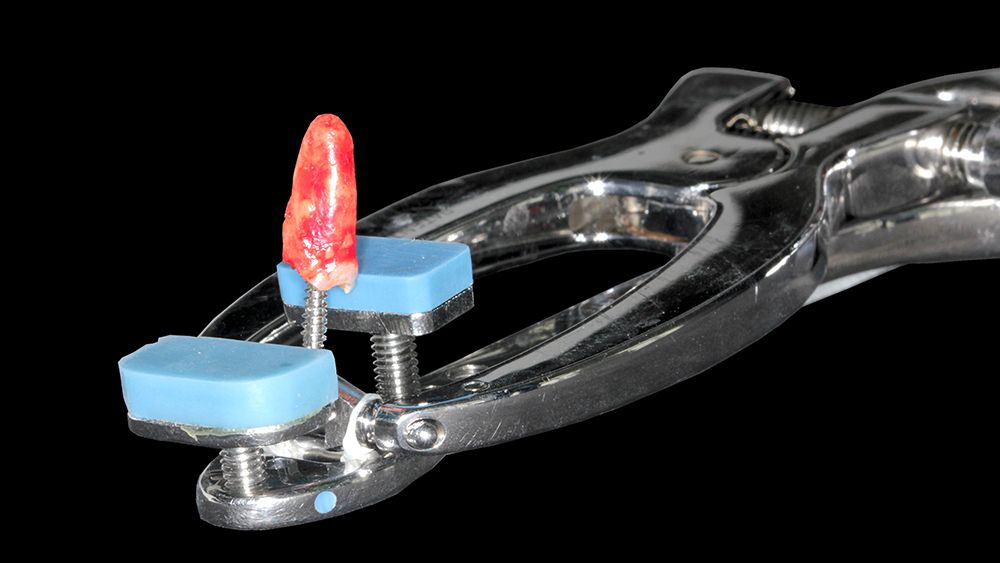
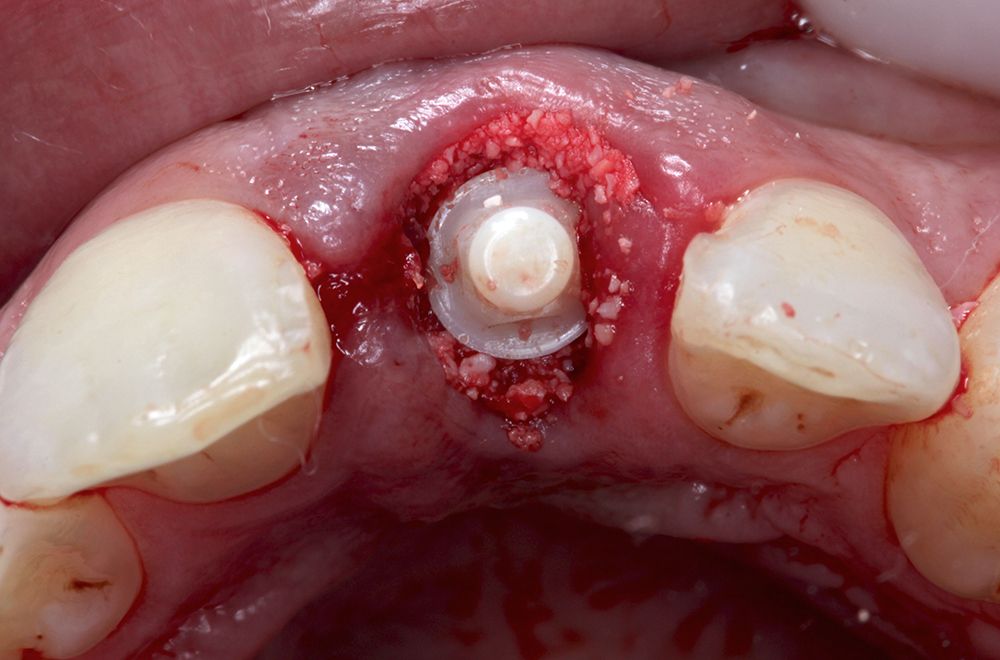
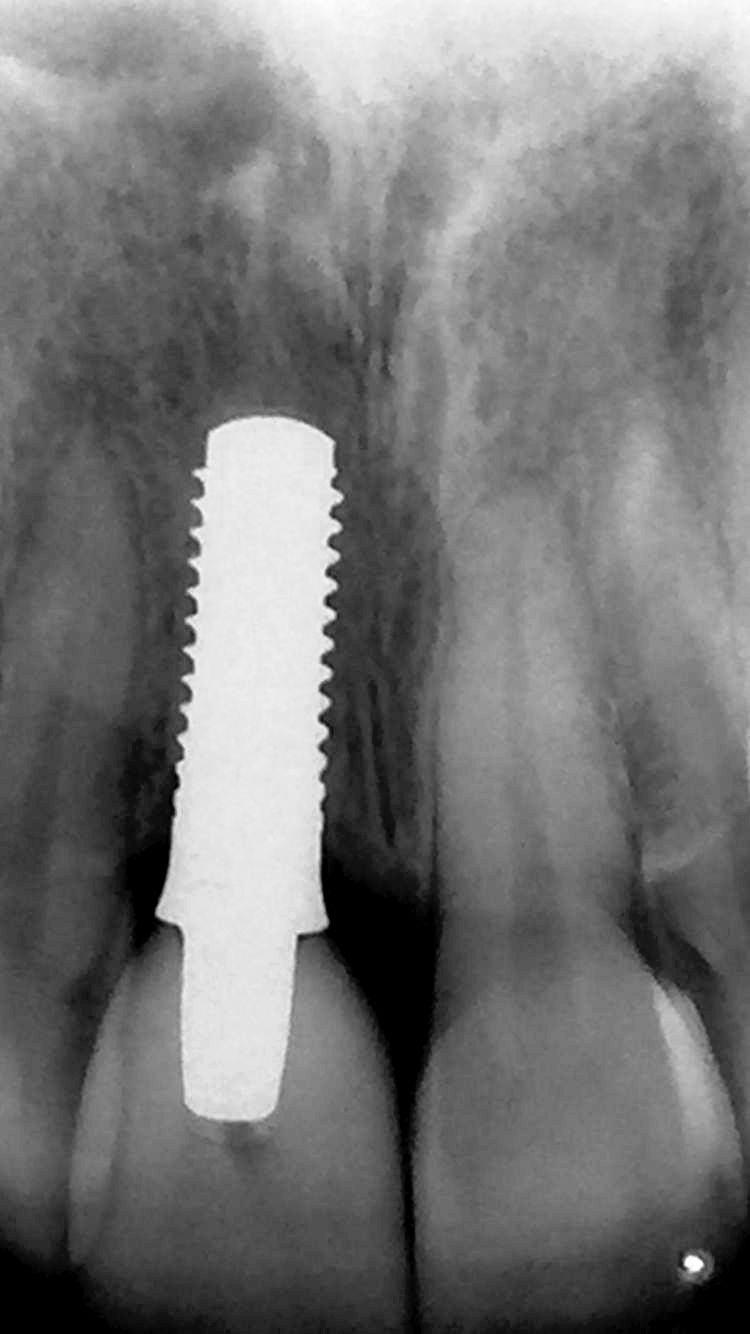
A female patient came to private consultation presenting fracture of tooth 11. The patient presented good overall oral hygiene with healthy-looking gingival tissue, though with thin gingival type, and absence of other prostheses or restorations in the aesthetic region. The tomographic exam confirmed the fracture and showed remaining bone structures sufficient for immediate implant placement (Figs. 1-2). Prior antibiotic therapy was prescribed with 1g of amoxicillin 1 hour before surgery in addition to 4mg of dexamethasone. The anaesthesia using lidocaine with epinephrine 1:100.000 was conducted. The extraction was performed with minimal trauma aiming to preserve the remaining thin buccal bone plate through the use of a tooth extractor (Exodent-Microplant, São Paulo - Brazil). Figures 3 and 4 illustrate the positioning of the extractor with its intra-radicular attachment and the root being extracted. The drilling required for the selected zirconia implant (Pure Ceramic - Straumann, Basel - Switzerland) follows the same sequence of drills and rotation necessary for placing a similar implant in titanium (Fig. 5). Figure 6 illustrates the alignment pin of the implant. In this one-piece implant system (Fig. 7) the positioner is customized according to the diameter and length of the abutment. The prosthesis must be cement-retained. The presence of apical bone, confirmed by pre-operative computed tomography, allowed adequate primary stability of the implant, which was placed in a prosthetically favourable position (Figs. 8-9). The gap located between the thin buccal bone plate and the implant was then filled with small-particle bovine xenograft (Bio-Oss, Geistlish-Pharma, Wolhusen – Switzerland) (Fig. 10). To make the temporary restoration, a crown was milled in PMMA and it was fitted in place based on a prior intra-oral scan. The temporary crown was relined with acrylic resin so as to obtain a cervical contour that would guarantee an emergence profile suitable for full sealing of the grafted socket and accommodation of the gingival tissue around it (Fig. 11). Cementation was done with Temp-Bond (3M ESP, Sumaré - Brazil) using an abutment analogue to remove the excess cement outside the mouth, thereby avoiding cement draining and possible graft contamination. Figure 12 illustrates how gingival zenith is maintained, keeping the same alignment as the adjacent tooth, as well as maintenance of the papilla, without the need of suturing. The impression taking of the implant occurred after a 2-month period. A smile design study was made, which showed the necessary adaptation of the adjacent teeth through injection-molded metal-free veneer laminates (Fig. 13). The implant crown was also made using injected ceramic (Fig. 14). The one year follow-up shows stability of the peri-implant soft tissues (Figs. 15-16).










Discussion
Wide dissemination of aesthetic dentistry brings an increasing number of young patients to the dental offices. This profile of patient, in search of the ideal aesthetic in the shortest time possible, often prefers to complete a treatment with implant restoration, rather than being submitted to orthodontic, endodontic and prostheses treatments. This clinical case report demonstrates the possibility of obtaining a high level of aesthetics in tooth restoration using a zirconia implant in patients with this profile. Zirconia has been widely used in prosthetics laboratories to make restoration viable in cases with high aesthetic demand, with biocompatibility and high affinity with the adjacent soft tissues. In patients with thin gingival phenotype, where gingival translucency may lead to discoloration of the gingival margin due to the grey colour of titanium, the alternative of a zirconia component is becoming increasingly popular. The use of zirconia implants or abutments may reduce the need for gingival graft techniques, which minimises surgical morbidity for the patient and speeds up case completion 6-8,15. Spies et al., 201616 showed that zirconia allows for aesthetic restoration with at least the same adaptation characteristics as with a titanium component. Nevertheless, Thoma et al., 201517 reported a major incidence of fracture of zirconia components in a study where these were compared to conventional titanium abutments. However, in a prospective study of one-piece restorations in 42 patients, Gahlert et al., 201518 demonstrated a success rate of 97.6% after 12 months using a one-piece zirconia implant (Pure Ceramic - Straumann, Basel - Switzerland), which makes the use of a second component screwed to the implant unnecessary. This indicates greater reliability of one-piece ceramic implants compared to two-piece implants or even those made of alumina, which, in a literature review carried out by Andreiotelli et al. 200919, showed only a 23% success rate after 10 years of follow-up. Nevertheless, it is fair to consider that the use of one-piece implants could lead to some technical difficulty since they do not allow, for example, the insertion of an angled abutment. In relation to zirconia aging, Cattani-Lorente et al. 201420 verified that surface treatment of zirconia implants may enhance hydrothermal degradation, which would affect the hardness and elasticity of zirconia. In the same way, Basílio et al.201621 tested in vitro the hydrothermal degradation of zirconia abutments, simulating effects of early aging. Assessing the stability and resistance to fracture in the micro-structure of zirconia components, the authors reported that aging conditions significantly reduced resistance to fracture (P<.001). They concluded that resistance to fracture and stability of zirconia abutments were susceptible to hydrothermal and mechanical conditions. However, ageing conditions did not alter the microstructure of the zirconia surface. Along these research field, resistance studies began to be designed to assess zirconia implants. Osman et al., 201322 described that zirconia has levels of hardness and resistance similar to those of the titanium alloy currently used to make dental implants. Accordingly, zirconia implants are considered a potential substitute for conventional titanium implants when there is a need for highly aesthetic treatment. This implant is made using zirconia (ZrO2), which normally then undergoes treatment surface with abrasive jet and acid conditioning, similar to those used in titanium. Gahlert et al., 201223, corroborating Thoma et al., 201517, presented a histomorphometric study in which zirconia implants maintain the same characteristics and quality of osseointegration as titanium implants, with no significant difference in Bone-Implant Contact (BIC), 78.6% ± 17.3% and 87.9% ± 13.6% respectively. In a similar vein, Bormann et al. 201213 carried out a comparative study to assess the difference between the removal torque of zirconia implants as compared to that of titanium. After assessing 102 implants, the authors reported no statistical difference between the materials. Another characteristic of zirconia is its low affinity with biofilm, which allows hygiene to be maintained, even after surface treatment to improve osseointegration24. This fact may be related to the low rate of bone remodeling, of around 1.02mm, after 12 months18. Added to this is the fact that the distance between the peri-implant mucosa and the apical termination of the epithelial barrier is less for zirconia than for titanium25. In a recent research, Hosoki et al., 201626 reported the allergic sensitivity of some patients to titanium, contraindicating restoration using conventional implants. In such cases, corroborating Oliva et al., 201027, the authors suggest the use of an implant made exclusively of zirconia as an alternative treatment. The use of a zirconia implant can therefore be considered for treatment not only in terms of high aesthetic requirements, but also to provide the patient with some choice.
Conclusion
Despite the surgical technical sensitivity, the zirconia implant enabled resolution of the aesthetic issues in this clinical case of thin gingival phenotype, without the use of gingival grafts.