
In Germany alone, more than 30,000 allogenic bone transplantations are performed every year. In the field of dental implantology, allogenic bone grafts have recently become of greater importance, based on their unlimited availability and their advantage of having a less invasive procedure in comparison to autologous bone augmentations1. Processed allogenic bone and autologous tissue do not exhibit any differences in their immunological compatibility. Furthermore, no circulating antibodies can be detected in the blood plasma of treated patients2. Beyond that, it has been shown on a radiological, histological and morphological basis that autologous bone and allografts do not differ in the final phase of incorporation3-6.
Although having certified production processes ensures the highest safety standards, isolated cases of disease transmissions described in the literature still lead to uncertainties by the clinical users. In these cases, "fresh frozen bone" allogenic material had been used, which has no current relevance in the dental field in many countries including Germany. In Germany, mainly two pharmaceutical forms for decellularized, allogenic material are used for procedures in oral surgery and implantology today:
- mineralized processed bone allograft (MPBA), with major relevance in implantology7
- demineralized freeze-dried bone allograft (DFDBA), with minor relevance in implantology



European directives harmonize quality standards
"Cells+Tissuebank Austria" (C+TBA), the biggest tissue bank in Austria, is a nonprofit organization specialized in human bone tissue. Martin Hennes highlights that "all processed transplants originate from donor tissue procured in Austria and Germany, countries which have implemented the European directives into national law and are rigorously controlling its abidance". "Tissue procurement follows standardized protocols. All tissue donations are based on a written donor consent after thorough donor assessment (anamnesis) with highly selective exclusion criteria", explains Hennes and adds: "All donations are done on a voluntary, non-remunerated basis."
Before 2004, national laws have secured the quality requirements for tissue donations. The year 2004 marked a milestone, with the harmonization of different national regulations by the European Parliament and the Council of the European Union within the scope of increasing the safety of allograft use. A first directive determined how cells and tissue should be handled8. Two years later another directive for tissue banks and procurement centers followed9: While procurement centers are responsible for the tissue procurement, tissue testing and tissue release for processing; the remaining processes are the responsibility of the tissue bank. This includes the tissue processing, storage and distribution of cells and tissues. C+TBA is regulated by the Austrian Tissue Law (Gewebesicherheitsgesetz, GSG), which is the transposition of the two European directives into national Austrian law and has been in force since 2008.
"Tissue banks are strictly regulated", explains Hennes. "This means that they need a regulatory approval and are – as in the case of C+TBA – subject to inspection by a public authority every two years, namely the Austrian Agency for Health and Food Safety on behalf of the Austrian Federal Office for Safety in Health Care".
It is a long way between the donation of the tissue via its processing to the final product for the patient. "To establish a tissue bank is not a trivial matter, it takes some time", reasons Hennes and explains: "In Europe there are just a few tissue banks, which, similar to the C+TBA, accompany, organize and control the whole process, starting from tissue procurement to its processing into allogenic transplants, up to its final Europe-wide distribution via important partner companies."
Controlled procurement and gentle cleaning process
The cancellous bone material originates from living human donors after explantation of the femoral head during hip endoprosthesis surgery. "This represents 99.5% of all tissue which is processed at the C+TBA." C+TBA collaborates with around 60 clinics in Austria and Germany. All tissue donations are performed according to contracts between these clinics and C+TBA. A major requirement for the tissue donation and blood testing is the written patient consent. Hennes: "After serological and microbiological testing, the donor tissue is released for the gentle cleaning process which is done with the highest quality standards (AlloTec® process). The processing of 50 femoral heads takes a whole week."

Fig. 4: To guarantee the highest safety, extensive technical requirements need to be fulfilled.
Overview of the AlloTec® process (Step 1 to 7):
1. Donors are selected after thorough anamnesis and health examination. After approval as a donor, the donor tissue is extracted under controlled conditions by an experienced surgical team in a specific clinic. After extraction and following radiological and clinical examination of the tissue by the responsible surgeon, the femoral head is shipped to C+TBA in a cooled and temperature-monitored package.
2. A range of serological tests are performed, e.g. antibody screening (Ak) and nucleic acid tests (NAT). Where it is not possible to detect the antibodies associated with core and surface antigens of Hepatitis- (HBs, HBc) and HI-viruses (Ag p-24), the NAT method is able to detect the antigens of these viruses. Hennes: "This takes around 48 to 72 hours. The tissue processing starts only after having assessed the diagnostic findings and final clearance".
3. After crude removal of surrounding soft tissue, fat and cartilage, the donor tissue is manufactured into its final shape (e.g. blocks, rings, granules). An ultrasonic bath is used to remove blood, cells and tissue components, but mainly to promote the removal of fat from the cancellous structure of the bone, improving the penetration of subsequent substances.
4. The processing is done under cleanroom conditions. The Allotec® process removes any residual fat, denatures non-collagenic proteins, inactivates potential viruses and destroys bacteria. (Depletion of at least 6 log levels).
Cleaning with volatile reagents
"We do not use aggressive chemicals. That’s the major point", emphasizes Hennes. "This is the main difference between us and other tissue banks. C+TBA uses volatile reagents like ether, alcohol and water for injection (WFI). Because of the characteristics of these reagents and the individual processing steps there is no risk whatsoever that any residues end up in the patient and lead to adverse events." Cleaning with the AlloTec® process preserves the biomechanical and biological properties related to bone regeneration.
5. During the cleaning process and after treatment with the ultrasonic bath, remaining cells are eluted, non-collagenic proteins are denatured and antigenic and immunogenic potential is reduced. Most notably potential viruses are inactivated and any remaining bacteria are destroyed. The following oxidative treatment denatures persisting soluble proteins, inactivates non-enveloped viruses and bacterial endospores and reduces any potential antigenicity to a minimum, whereas non-soluble collagen remains intact during this step.
6. After the cleaning process with volatile reagents the tissue is lyophilized. During this gentle dehydration technique, frozen tissue water is sublimated from solid phase to gas phase (residual moisture ≤10%, thereby preserving the natural structure of the tissue.
7. After chemical processing, the allograft is double packed and sterilized for a final time by gamma-irradiation (minimum does of 25kGy). This guarantees a pharmaceutical sterility assurance level (SAL) of 10–6 (This means that in one million sales units a maximum of one germ is allowed to be included) and a gentle sterilization of the final product and its packaging without any structural or functional constraints. "Double packing and final sterilization by gamma-irradiation guarantees a 5-year shelf-life at room temperature." "Only after having received all data regarding the sterilization process and being able to ensure the product sterility, we release the products."
Limited availability: Transplants from multi-organ donors
There are transplants which can only be gained from multi-organ donors. This concerns two botiss products (maxgraft® block cortico-cancellous and maxgraft® cortico). "These cortical and cortico-cancellous allografts originate from donors whose femur and distal end of the tibia are explanted within a maximum of 24 hours post mortem after thorough medical examination". "Organ donations do not have any higher safety risk than living donations, as explantation and testing procedures are the same", argues Hennes against the controversial discussion about this topic. "Who can and can’t be a donor is regulated in Europe by national transplantation laws. "In Germany donors need to give active consent, whereas in Austria everybody is a donor who does not actively opt-out and is registered in an opt-out data base. In other European countries, consent must also be given by the nearest relatives. Although there is this opt-out system for organ donation in Austria the mobile tissue extraction team of C+TBA only organize around 15 donations per year on average.’
There is a safe traceability regarding both living donations and organ donations. "The traceability is documented via the SEC Code (Single European Code) for tissue on every transplant", explains Hennes. Until now, in more than 100,000 transplantations using allogenic grafts from C+TBA, no critical incidents were reported to C+TBA. Hennes: "The quality process is well-proven and is a prerequisite for the clinical success."
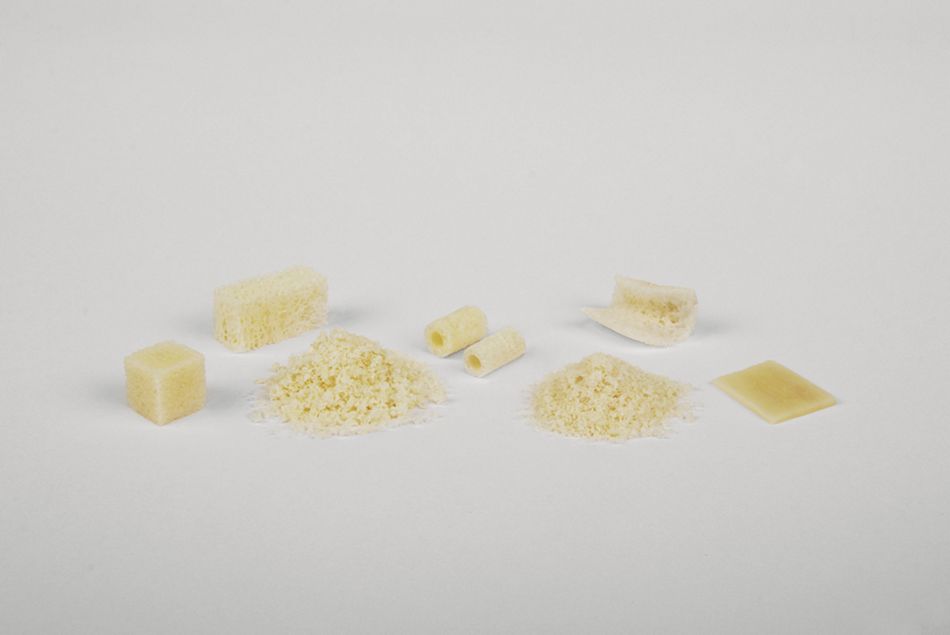
Fig. 5: Allografts for dental application (maxgraft®, botiss biomaterials GmbH)
Outlook-Safety, consolidation, technology transfer
The production process which is certified in Europe ensures the highest quality standards. "The existing situation in Europe is a benchmark". In North America, the basic requirements are different. There, the system is based on organ donations, which affects the opportunities for transplant procurement. There will be no change in the C+TBA quality standard, and Hennes concludes: "First, our transplants have the biological active, regenerative component, which supports natural bone remodeling. Second, they offer an easy handling like medical devices and are available with reliability. Third, our transplants are safe as pharmaceutical products, which documents the very fact of the product approval in Germany. Biologically active, easy to handle, available and safe – that is what donors, clinical users and first and foremost patients can expect of allogenic transplants in Europe today.