Introduction
Furthermore, due to the pattern of bone resorption and the presence of the alveolar nerve, prosthetic rehabilitation of resorbed edentulous mandible is difficult. 2
Several studies have shown that implant-supported overdentures in the mandible are a successful therapeutic technique, particularly in individuals with substantial residual bone loss, where retention and stability need to be improved. 3,4
The following case report describes the use of the ø2.4 mm Straumann® Mini Implant in a patient with limited bone availability in the lower jaw. The Straumann® Mini Implant System, made of Roxolid® with the SLA® surface, offers one-piece Tissue Level implants with an Optiloc® prosthetic connection.
Initial situation
A systemically healthy, non-smoking 64-year-old female came to our clinic requesting a solution to improve her smile esthetics and masticatory function. She stated: “I am looking for a non-invasive solution for my mouth. I no longer tolerate the adhesive glue to hold the lower denture in place, and continuous direct and indirect relines have been unsuccessful.” She reported wearing full-arch dentures in the upper jaw for 15 years and in the lower jaw for 40 years.
The extraoral examination showed a lack of support for the lips, and this was reflected in the patient's profile.
The intraoral examination revealed fully edentulous maxillary and mandibular arches. In the lower jaw, the shape of the alveolar processes in the anterior zone was round and adequate in height and width (Class III, Cawood and Howell Classification). On the other hand, in the posterior zone, a knife-edged ridge form was encountered, adequate in height and inadequate in width (Class IV, Cawood and Howell Classification). In addition, the width of keratinized mucosa was minimal (Fig. 1).

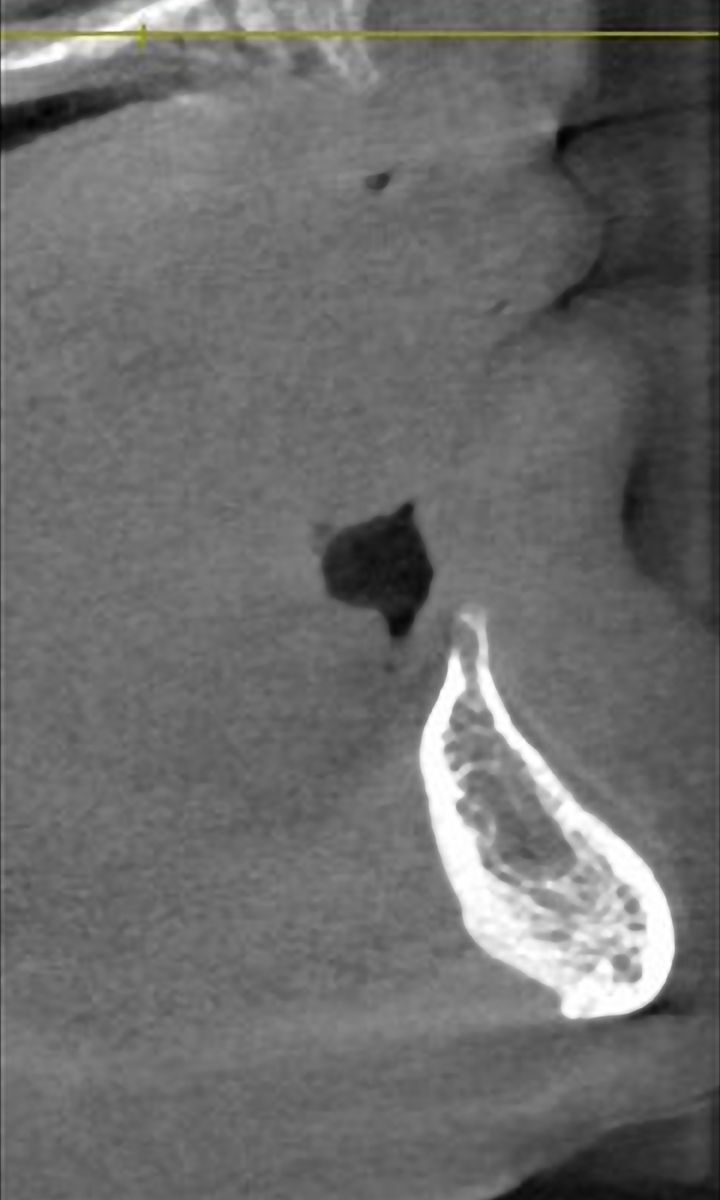
The radiographic examination showed generalized vertical bone resorption with very limited bone availability in the posterior area of the lower jaw (Fig. 2).