

Introduction
The prosthetic workflow was based on using the one model technique allowing to derive the esthetic and functional criteria of the fixed temporary and final prosthesis from information acquired in the presurgical phase without requiring post-placement impressions or maxillomandibular registration 6,7. This report describes the application of this technique using a digital-analog hybrid workflow.
Initial situation
A 58-year-old male, non-smoker patient in good general health (ASA 1 class) presented in our clinic with a chief complaint of pain and mobility of his existing prosthesis. He reported difficulties in chewing and unsatisfactory esthetics. Extra-oral and esthetic examination revealed a reversed curve of smile and a low smile line concealing the gingival margin, except for the right buccal corridor (Fig. 1).
- Fig. 1 Patient prior treatment – LEFT: facial aesthetics and smile line, RIGHT: profile view indicating the visibility of the gingival margins in the right quadrant
- Fig. 1 Patient prior treatment – LEFT: facial aesthetics and smile line, RIGHT: profile view indicating the visibility of the gingival margins in the right quadrant


Intraoral examination revealed the presence of an upper and a failing lower fixed tooth-borne resin prosthesis. The latter was fractured, resulting in mobility and buccal displacement of the right segment in the fourth quadrant. Oral examination indicated a severe generalized stage IV periodontitis associated with poor oral hygiene and bleeding on probing, progressed gingival recession, exposed root surfaces, loss of interdental papillae, and gingival hyperplasia in the lower frontal segment (Fig. 2).
Diagnostic cone-beam computer tomography (CBCT) scans revealed the presence of extensive horizontal bone loss with deep infrabony components. The dental status was considered insufficient for restoration with an adequate prognosis. The alveolar anatomic dimensions were adequate to allow for immediate implant therapy.
- Fig. 2. Pretreatment dental and radiographic status – LEFT: intraoral frontal retracted view revealing the fractured mandibular prosthesis and dental status compromised by periodontitis, RIGHT: panoramic radiograph illustrating the presence of excessive horizontal bone loss with deep infrabony components.
- Fig. 2. Pretreatment dental and radiographic status – LEFT: intraoral frontal retracted view revealing the fractured mandibular prosthesis and dental status compromised by periodontitis, RIGHT: panoramic radiograph illustrating the presence of excessive horizontal bone loss with deep infrabony components.


The diagnosis and therapeutic alternatives were shared with the patient using a set of intraoral and extraoral photos, an intraoral scan, and the CBCT scan as communication tools. From the different treatment alternatives, the patient expressed his preference for a fixed full-arch rehabilitation, avoiding any treatment periods without restoration or employing transient removable restoration.
Based on his specific requests, a fixed full-arch restoration with a maxillary metal-ceramic and mandibular metal-composite hybrid prosthesis using an immediate procedure was proposed, economically quantified, and consented by the patient.
Treatment planning
The treatment plan for the patient was based on an immediate bimaxillary procedure involving immediate placement, loading, and provisionalization with a prefabricated fiber-reinforced prosthesis; the delivery of the final definitive prosthesis was planned 6 months after implant placement.
The procedure was carried out using a combined analog-digital workflow following the one-model technique. This technique was developed to allow immediate placement of a screw-retained prefabricated prosthesis based on wax-ups that are exclusively based on diagnostic information acquired pre-surgically and without the need for impressions or registrations of the maxillomandibular relationship post-implant placement6,7. The workflow applied for the described cases was optimized using digital impressions, and CAD/CAM printed casts and guides.
In brief, a preliminary wax-up was obtained from a full-mouth intraoral scan in occlusion (Fig. 3);
- Fig. 3 Full mouth intraoral scan of the patient's conventional restoration and residual dentition in occlusion as a basis for the preliminary wax-up.

The new relationships between the upper lip and face were designed using the preliminary wax-up and evaluated using a milled mockup positioned on top of the existing prosthesis (Fig. 4).
- Fig. 4 Evaluation of the aesthetic appearance of the future planned restoration in relation to the patient's face and lip line using a digitally designed and milled mockup.
- Fig. 4 Evaluation of the aesthetic appearance of the future planned restoration in relation to the patient's face and lip line using a digitally designed and milled mockup.


Based on the information of the mockup, an analog wax-up of the upper prosthesis using conventional laboratory techniques was prepared (Fig. 5).
- Fig. 5 Printed master cast of the patient's existing restoration.
- Fig. 5 Printed master cast with the mockup representing the positions of crowns in the future restoration.
- Fig. 5 Wax-up of the future restoration based on bite registration and reference planes of the patient wearing the mockup.



As illustrated by the image sequence in Figure 6, a wax-up of the lower prosthesis was fabricated in adequate functional relationships with the upper arch. The wax-ups were scanned using a laboratory scanner, and the resulting digital wax-ups were used to design the upper and lower provisional prosthesis with corresponding cervical soft tissue interfacing contours. The resulting models were used to mill the fiber-reinforced provisional.
- Fig. 6 Completed wax-up of the upper and lower future prosthesis using conventional laboratory techniques.
- Fig. 6 Resulting digital wax-ups from laboratory scans of the prosthesis in the process of adapting the cervical soft tissue interfacing aspects for the provisional restoration (maxilla).
- Fig. 6 Milled provisional prosthesis.



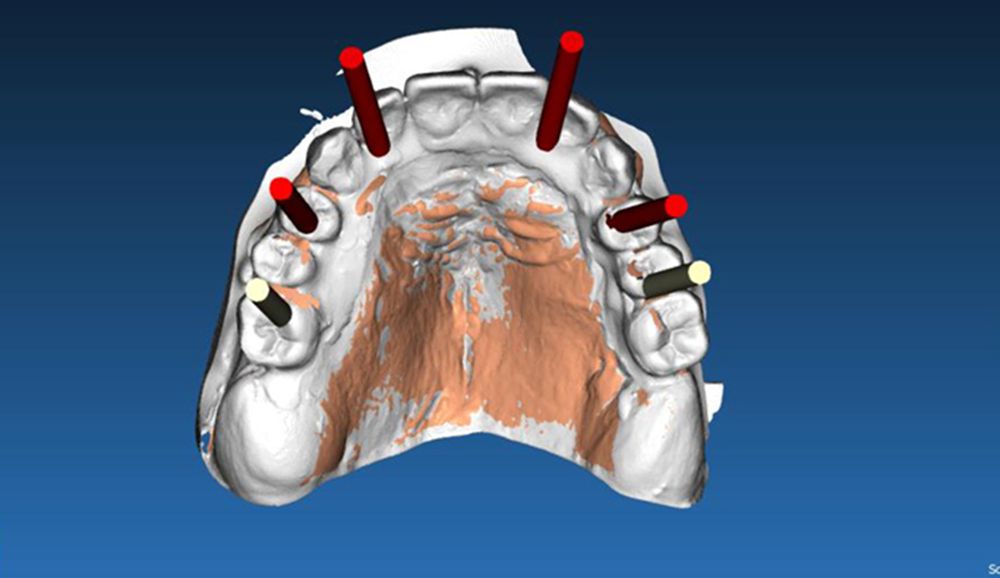
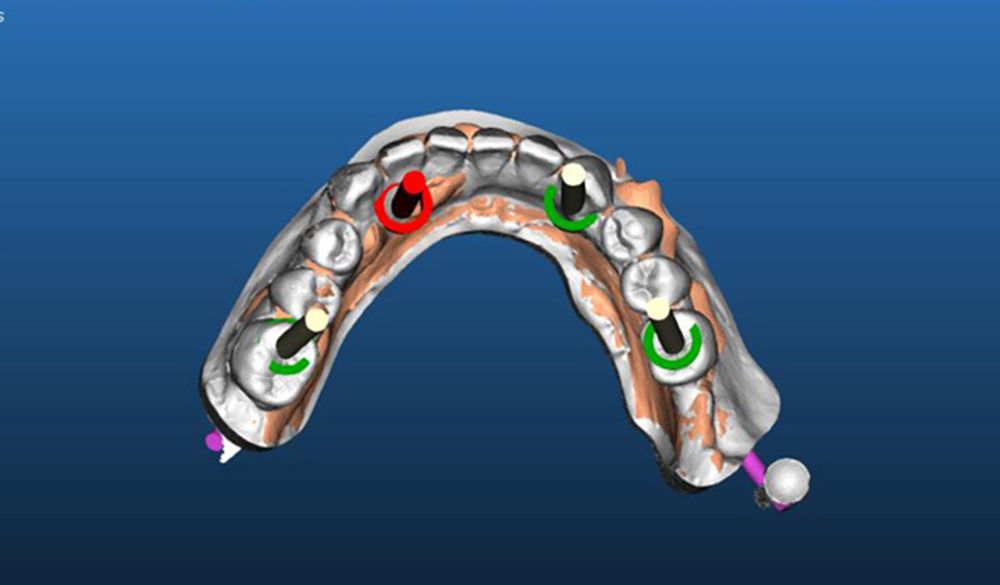
Next, the STL files of the upper and lower digital wax-ups were superimposed with the DICOM files of the CBCT scans to deliver the virtual implant planning model. Fig. 7 illustrates the detailed planning of the implant restoration based on 6 maxillary and 4 mandibular TLX®-Roxolid®-SLActive® Implants. Planning was performed in coDiagnostiX® under consideration of the future prosthetic restorations and local alveolar anatomy. The treatment strategy also considered the patient's periodontal preconditions, implying a more pronounced demand for hygiene maintenance and long-term biologic tissue stability. The novel TLX® implant represented the ideal tool to meet these requirements and achieve an optimal level of primary stability as part of the immediate protocol.
- Fig. 7 Virtual implant planning of the maxilla (LEFT) and the mandible (RIGHT).
- Fig. 7 Virtual implant planning of the maxilla (LEFT) and the mandible (RIGHT).
The upper and lower prosthesis, two lower and one upper surgical guides for implant placement, and one upper and one lower resin transfer plate to register the actual implant positions in the final prosthetic model were delivered to the clinic on the day of surgery.
Surgical procedure
Implant placement was performed using a "simplified, guided surgical technique". Specifically, surgical guides were only used with initial drills (up to Ø 3.2 mm) to prepare the osteotomy to the defined depth. The surgical guides were then removed, mucoperiosteal flaps were elevated, and bone reduction was performed to flatten the alveolar crest, eliminate the infra bony defects and increase the restorative space. Subsequently, the osteotomies were finalized conventionally and freehand—this strategy allowed to assess the bone quality during the osteotomy preparation and adapt the surgical technique accordingly. Due to poor bone quality in the distal left maxilla, e.g., it was decided to underprepare the osteotomy using an osteotome technique resulting in sufficient primary stability of the TLX implant (Ø4.5 x 8mm) to allow for immediate loading (Fig. 8).
- Fig. 8 Illustration of the maxillary surgical procedure. The osteotomy positions and depths were defined using guided initial drilling up to diameter 3.2 prior to flap elevation and bone reduction.
- Fig. 8 Illustration of the maxillary surgical procedure. Finalization of an underprepared osteotomy due to poor bone quality in the distal left maxillary aspect.
- Fig. 8 Illustration of the maxillary surgical procedure. Placement of a Ø4.5 TLX implant.
- Fig. 8 Illustration of the maxillary surgical procedure. Completed implant placement in the maxilla.




Directly after implant placement, the implant positions were recorded by mounting transfer copings to the implants and fusing them to the maxillary transfer resin plate using self-curing acrylic (Fig. 9). Specific care was taken during positioning the acrylic transfer plate into the reference palatal vault.
- Fig. 9: Registration of implant positions by fusing transfer copings to the transfer plate after stabilizing and aligning it with the palatal vault.

Two surgical guides were used for the mandibular procedure. The first guide for placing the two anterior implants was retained by anterior anchoring pins. This guide was further supported by posterior teeth left temporarily in situ, which served as a reference for positioning the guide. The second guide was positioned using the same pin holes used for the first guide and was used for the osteotomy preparation of the distal implants after extraction of residual teeth and bone reduction. Distal implants were placed freehand (Fig. 10).
The actual mandibular implant positions were transferred to the prosthetic models using a transfer plate for the anterior implants on the one hand and a splint of the transfer copings of all 4 implants on the other hand. Specifically, the transfer plate used the posterior teeth left in situ as a landmark for positional reference and was fused to transfer copings mounted on the two anterior implants before distal implant placement. The splinted transfer copings, on the other hand, were obtained by connecting all four transfer copings mounted on the completed implant base using self-curing acrylic and with anterior implants for positional reference.
- Fig. 10 Surgical guide and implant placement in the mandible. Illustration of the second surgical guide used for the placement of distal implants.
- Fig. 10 Surgical guide and implant placement in the mandible. Resulting situation after tooth removal, bone reduction, and implant placement.



Want to stay up to date?
youTooth.com is THE PLACE TO BE IN DENTISTRY – subscribe now and receive our monthly newsletter on top hot topics from the world of modern dentistry.
Prosthetic procedure
The prefabricated, fiber-reinforced wax-up was converted into a screw-retained provisional prosthesis using the one model technique. This technique employed the same models for the wax-up/design, construction, and to convert the wax-up into the screw-retained temporary prosthesis. The procedure avoided the need to take impressions during surgery and record the inter-maxillary relationship and vertical dimension after surgery. The implant analogs were incorporated into the required models by utilizing the transfer resin splints with the same sequence applied in the mouth to connect the transfer copings to the transfer plate.
For the maxillary model, space was first created in the alveolar process of the model. Next, the corresponding fused resin plate and transfer copings were equipped with analogs and positioned on the model using the palatal vault as a reference. The analogs were next incorporated with plaster into the model.
- Fig. 11 Transfer of maxillary implant positions to the initial model. Printed maxillary master cast after opening the implant-bearing segments of the alveolar process.
- Fig. 11 Transfer of maxillary implant positions to the initial model. Alignment of the splinted transfer copings fused to the transfer plate in the palatal vault.
- Fig. 11 Transfer of maxillary implant positions to the initial model. Finalized plaster cast model with non-engaging titanium provisional abutments.



The transfer of the implant positions to the mandibular model was achieved accordingly. Specifically, the anterior segments of the printed cast were removed to allow for the positioning of the mandibular transfer plate splinted with transfer copings of the anterior implants. Next, the two transfer copings were equipped with implant analogs; the transfer plate was correctly oriented on the cast using the posterior teeth as reference and plaster cast to the model. After removing this first splint, the anterior positions of the resin splint comprising all 4 transfer copings were equipped with implant analogs. They were mounted on the reference anterior implants of the model, and the two posterior analogs were plaster cast to the model. Transfer copings were then replaced by non-engaging temporary Titanium abutments (Fig. 12).
- Fig. 12 Transfer of mandibular implant positions to the initial model. Transfer of anterior implant positions using posterior teeth as reference for the alignment of the transfer plate.
- Fig. 12 Transfer of mandibular implant positions to the initial model. Transfer of posterior implant positions using the complete splint with anterior implant positions as reference.


Next, the titanium copings were customized and incorporated into the prefabricated provisional prosthesis. Occlusion with the opposing prosthesis was used to correctly orient the individual prosthesis during alignment with the model (Fig. 13).
- Fig. 13 Incorporation of Titanium copings into the prefabricated prosthesis. Alignment of the upper and lower prosthesis on the printed master cast.
- Fig. 13: Incorporation of Titanium copings into the prefabricated prosthesis. Frontal view of the provisional prosthesis mounted on the master cast.


Treatment outcomes
Figure 14 illustrates the clinical and radiographic outcomes after immediate provisionalization and after 2 weeks of healing, respectively. The provisional prosthesis was delivered two hours after surgery, followed by a slight occlusal adjustment. Healing was uneventful (Fig. 14)
- Fig. 14 Clinical and radiographic situation after provisional restoration. Frontal view immediately after provisional restoration.
- Fig. 14 Clinical and radiographic situation after provisional restoration. 2 weeks after surgery.
- Fig. 14: Clinical and radiographic situation after provisional restoration. Panoramic radiograph after delivery of the immediate provisional.



The esthetics of the provisional restoration and its relationship with the facial parameters were evaluated as overall satisfactory (Fig. 15)
- Fig. 15 Esthetic evaluation of the provisional restoration

The esthetic and functional parameters of the immediate prosthesis were considered optimal and used as a reference for fabricating the final prosthesis. The upper metal-ceramics and a lower metal-composite prosthesis were delivered 6 months post-surgery (Fig. 16).
- Fig. 16 Esthetic, clinical, and radiographic outcomes after delivery of the final prosthesis. Frontal view of the patient.
- Figure 16: Esthetic, clinical, and radiographic outcomes after delivery of the final prosthesis Frontal view of the final restoration in retracted view.
- Fig. 16 Esthetic, clinical, and radiographic outcomes after delivery of the final prosthesis. Panoramic radiograph 6 months post-surgery confirming adequate implant osseointegration.



References:
- Chrcanovic BR, Martins MD, Wennerberg A. Immediate Placement of Implants into Infected Sites: A Systematic Review: Immediate Implants in Infected Sites. Clinical Implant Dentistry and Related Research 2015; 17: e1–16.
- Alves CC, Correia AR, Neves M. Immediate implants and immediate loading in periodontally compromised patients-a 3-year prospective clinical study. Int J Periodontics Restorative Dent 2010; 30: 447–55.
- Javed F, Ahmed HB, Crespi R, Romanos GE. Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation. Interventional Medicine and Applied Science 2013; 5: 162–7.
- Buser D, Mericske-Stern R, Dula K, Lang NP. Clinical Experience with One-Stage, Non-Submerged Dental Implants. Adv Dent Res 1999; 13: 153–61.
- Cosola S, Marconcini S, Boccuzzi M, Menchini Fabris GB, Covani U, Peñarrocha-Diago M, Peñarrocha-Oltra D. Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review. IJERPH 2020; 17: 6920.
- Biscaro L, Ferlin P, Becattelli A, Vigolo P. Prosthetic procedure for simultaneous immediate loading of opposing edentulous arches. The Journal of Prosthetic Dentistry 2014; 112: 713–6.
- Biscaro L, Becattelli A, Poggio PM, Soattin M, Rossini F. The one-model technique: a new method for immediate loading with fixed prostheses in edentulous or potentially edentulous jaws. Int J Periodontics Restorative Dent 2009; 29: 307–13.