Why use the Straumann® Pro Arch solution with the new Straumann® BLX Implant System? To find out, we have asked active users to tell us by selecting the most valuable features of BLX when used in full-arch restorations and to share their opinions about the system with us.1
An immediate full-arch restoration is always a challenge for the whole treatment team. At the same time, it is an opportunity to provide an outstanding treatment that will considerably improve the patient’s quality of life and give them back their smile – provided that the necessary skills and the right tools are available.
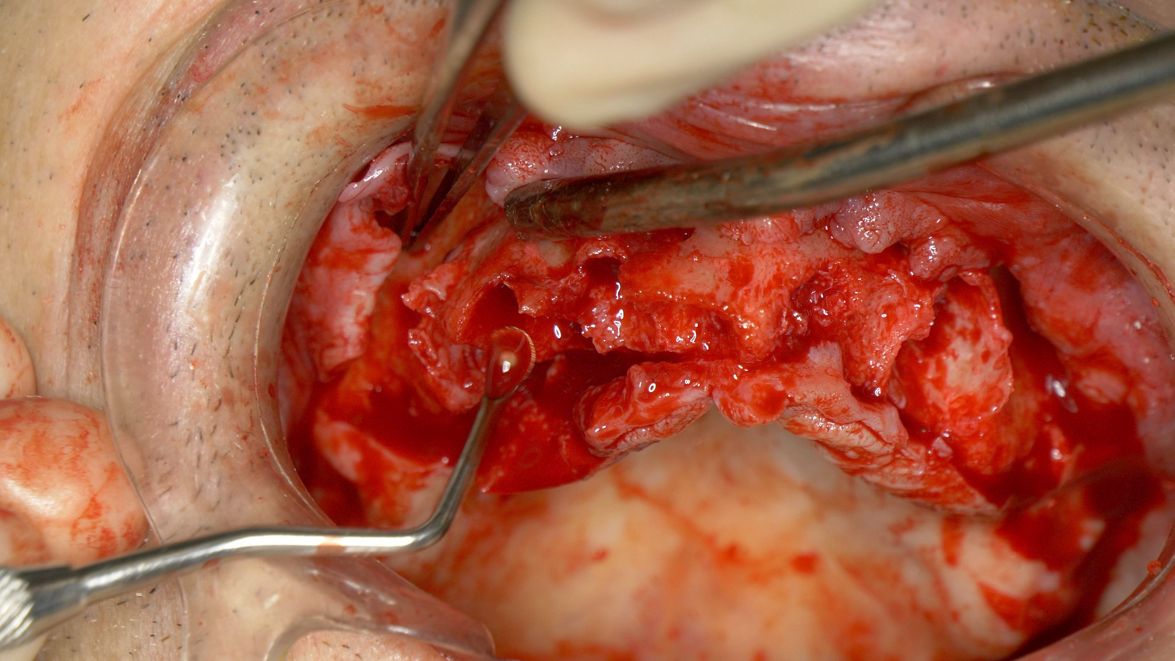
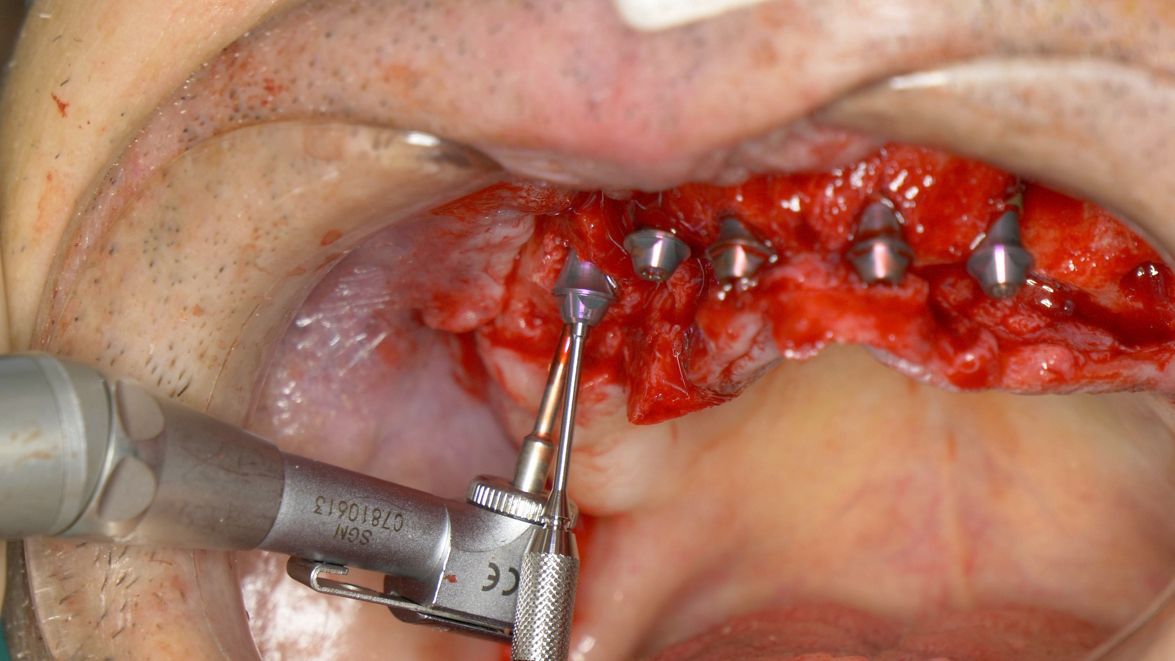
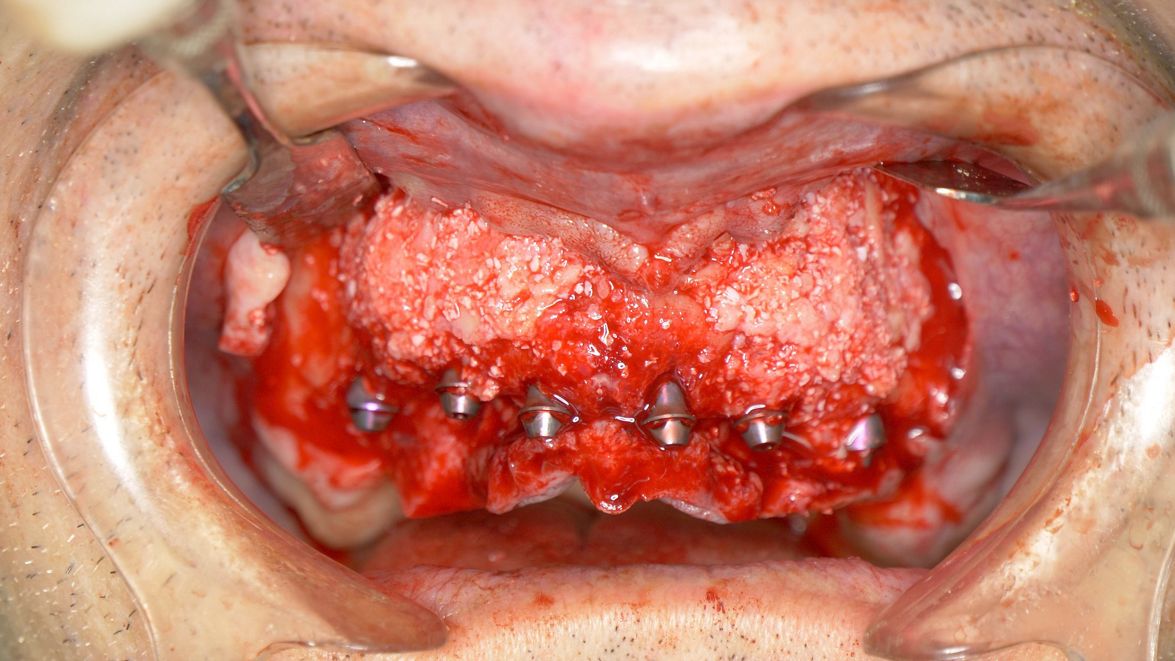
Immediate full-arch rehabilitation with Straumann® Pro Arch BLX (courtesy of J. Caramês)
The newly introduced BLX implant system enhances the Pro Arch solution for full-arch rehabilitations by offering a range of tools for the efficient, flexible, and confident treatment of such challenging cases. In this article, you will find a ranking of the most valuable features of Straumann® Pro Arch BLX based on a customer survey.
Reason #7: An optimized Screw-retained Abutment portfolio is available
Rounded and slim angulated abutments maximize the space for soft tissue. Efficient: the single connection system reduces the number of abutments while keeping all clinical options open. The SRA should be tightened with 35 Ncm – like all BLX final abutments.

.")
Reason #6: The 3.75 mm diameter implant is suitable for all indications
The slim core of the ∅ 3.75 mm implant and its fully tapered implant design enable for bone-preserving protocols applicable in all indications. Even more peace of mind is added through the high-performance mechanical properties of Straumann’s Roxolid® implant material.2
._.jpg?crop=0,8,772,434&wid=772 "Immediate full-arch rehabilitation in the soft bone using Straumann® BLX 3,75 mm from 6 mm till 12 mm in one case (courtesy of B. Sobczak).")
.jpg?crop=0,130,3363,1892&wid=1175 "Immediate full-arch rehabilitation using Straumann® BLX 3.75 mm implant in the soft bone (courtesy of L. Cuadrado).")
_1.JPG?crop=0,313,6000,3375&wid=1175 "Immediate full-arch rehabilitation using Straumann® BLX 3.75 mm implant with 10 mm length in the hard bone (courtesy of Dr. L. Swart and P. van Zyl).")
Reason #5: The SLActive® surface works even in compromised patients
SLActive®, Straumanns premium surface, enhances bone generation3 and reduces healing time4. Even compromised patients (irradiated or with diabetes) can be treated with evidence-based predictability and peace of mind3-9.

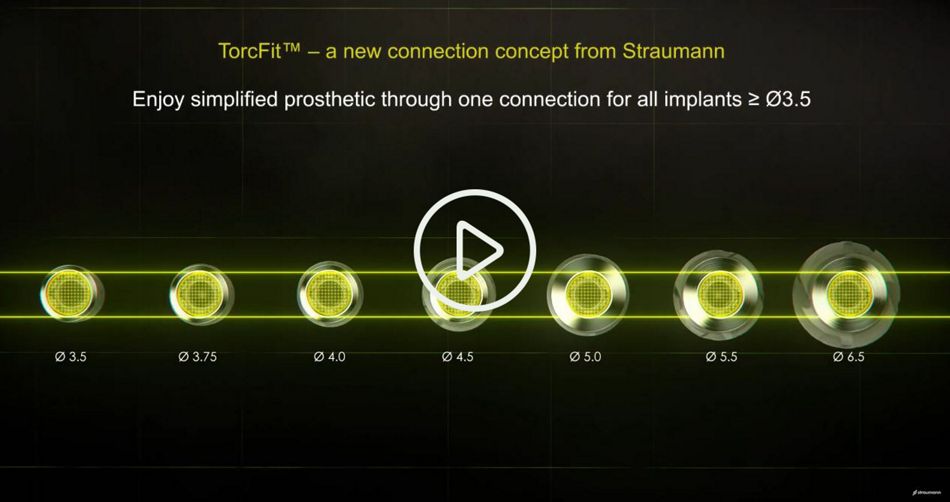
Reason #4: A broad implant range with only one single connection
A portfolio of 42 implants with just one single connection for all diameters means straightforward abutment choice, simple stock keeping and robust in-practice workflows.
Reason #3: One implant system can cover almost all full-arch indications
Straumann® BLX is designed for excellent primary stability in different bone qualities, thanks to its optimized thread design which is suitable for both mandible and maxilla. A wide range of available diameters (seven) and lengths (from 6 to 18 mm) offer high adaptability to the patient´s anatomy.

Reason #2: Dynamic bone management for enhanced control over insertion torque to achieve primary stability
Progressive double lead threads cut through hard bone and condense soft bone, for a uniform osseodensification along the full osteotomy. Bi-directional cutting elements enable back-forward turning and thus a controlled final insertion torque. Last but not least: the new VeloDrills with their cutting geometry design and a surface treatment that limits friction and facilitates debris extraction resulting in lower heat generation and a simplified drill protocol.

Reason #1: The implant design is optimized for primary stability
The BLX´s variable thread design, combined with a slim and tapered implant core, was developed for high primary stability in under-prepared sites – even in challenging situations. The reduced diameter neck helps to control the insertion torque and limits bone stress.

Straumann® Pro Arch BLX offers even more advantages not listed in this “Top 7” list, such as reduced drill steps, TorcFit™ connection (a tight 7° internal conical connection with 6 prosthetic positions for all implant diameters), Roxolid® material for reduced invasiveness, a small surgical cassette, and others. Learn what experienced clinicians have to tell (testimonials below)!
Interested to find out more and put Straumann® BLX to the test? Benefit from our special offer to experience new levels of efficiency, flexibility and confidence!